.avif)
Diastasis recti rehabilitation to restore core strength and abdominal function.
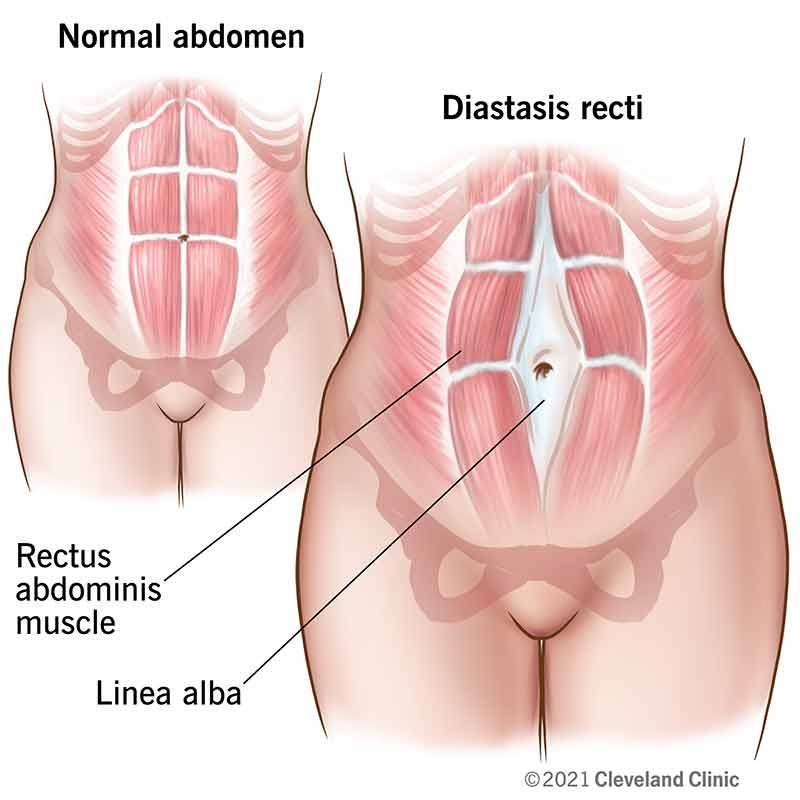
Diastasis Recti Abdominis (DRA) is defined as the separation of the right and left rectus abdominis muscle bellies as a result of partitioning or stretching at the linea alba. The linea alba is a strong fibrous cord, typically at least 10mm wide, that runs medially from the xiphoid process to the pubic symphysis. During pregnancy, particularly in the third trimester, increased levels of hormones such as relaxin and elastin soften this connective tissue, causing it to become flaccid and wider
Common Symptoms
The symptoms and experiences of individuals with Diastasis Recti Abdominis (DRA) are deeply rooted in the structural compromise of the abdominal wall and its role in trunk stabilization.
Prevalence
Diastasis recti abdominis (DRA) is most frequently seen secondary to pregnancy, with a steady increase in incidence as pregnancy advances toward a peak in the third trimester. Research indicates that approximately 70% of pregnant women are affected by the condition during this period. Immediately following childbirth, the prevalence remains high, affecting about 60% of postpartum women.
While small cases of diastasis may resolve naturally, many significant cases persist long-term if they are not treated. Statistics show that while 60% of women are affected immediately after birth, the condition remains evident in 30% of women at eight weeks postpartum. Without intervention, a pathological inter-recti distance has been shown to remain above normal values even six months after delivery.
Sources clarify that DRA is not gender-specific and can affect men as well as non-pregnant individuals. The condition is commonly associated with factors that increase intra-abdominal pressure, such as obesity, chronic obstructive pulmonary disease (COPD), multiple pregnancies, or a large amount of amniotic fluid. Other risk factors for developing a separation include:
The abdominal wall is composed of several muscles that work together to stabilize the trunk and support movement.
Key structures include:
When the linea alba becomes stretched, the rectus abdominis muscles separate, reducing the effectiveness of the abdominal wall.
Diastasis Recti Abdominis (DRA) is defined as the separation of the right and left rectus abdominis muscle bellies within their respective sheaths due to the partitioning or stretching of the linea alba. This fibrous cord, which runs from the xiphoid process to the pubic symphysis, typically measures at least 10mm wide but can become flaccid and wider under specific physiological stresses.
The development of this separation is driven by several interrelated factors:
Pregnancy-Related Changes
Increased Intra-Abdominal Pressure
Weak Deep Core Muscles
Successive and High-Load Pregnancies
Poor Movement Patterns and Improper Exercise
Physiotherapy is essential for the recovery of Diastasis Recti Abdominis (DRA) because a separation of the rectus muscles larger than 2 to 2.5 cm jeopardizes nearly every function of the abdominal wall, including posture, trunk stability, and respiration. Left untreated, the condition can persist for years, leading to a decreased quality of life and serious secondary complications such as chronic low back pain, urinary incontinence, and abdominal hernias.
Restoring Core Muscle Strength and Coordination
A primary goal of physiotherapy is the restoration of core strength and coordination, with a specific focus on the transversus abdominis (TA) muscle. Research indicates that isometric TA training—specifically drawing-in exercises—is more effective and gentler than traditional crunches at reducing the inter-recti distance (IRD). Physiotherapists guide patients in synchronizing these exercises with breathing (exhaling during the effort) to minimize intra-abdominal pressure, which is critical for protecting the weakened connective tissue during recovery.
Improving Abdominal Support and Stability
Proper abdominal muscle tension is required to hold internal organs at the correct height and maintain balanced pressure on the lumbar section of the spine, which prevents the deepening of lordosis. To support the abdominal wall while strength is being rebuilt, many clinicians utilize abdominal binders or splinting, particularly when the patient is performing strenuous activities or household chores that might otherwise cause the separation to worsen.
Correcting Posture and Movement Patterns
Physiotherapy is vital for correcting the postural imbalances often caused by a weakened core, such as hyperlordosis (increased lower back curve) and increased anteversion of the pelvis. Beyond specialized exercise, physiotherapists provide essential education on daily body mechanics, teaching patients the proper way to lift, breastfeed, and even get out of bed from a side-lying position to avoid placing excessive strain on the linea alba.
Guiding a Safe Return to Exercise
A specialist ensures a safe return to activity by implementing a progressive overload approach, moving carefully from supine exercises to sitting and eventually standing positions. They help patients identify and avoid abdominal "doming" or bulging, a sign that the core is unable to manage the current internal pressure and that the activity could potentially widen the separation. In the early stages of recovery, traditional exercises involving the oblique muscles (such as twisting) are often eliminated because their fascial connections to the rectus muscles can pull the separation further apart.
The recovery timeline for Diastasis Recti Abdominis (DRA) varies based on the size of the separation and individual adherence to a rehabilitation program, but the sources provide a clear framework for what to expect during this process.
Prognosis for Conservative Recovery
With consistent, specialized physical therapy, the prognosis is generally positive. Surveys of women’s health specialists show that clinicians help patients reduce significant separations to two finger widths or less 41% to 80% of the time. Furthermore, nearly 70% of therapists report a success rate between 41% and 100% in their overall plans of care. However, research indicates that while mild cases may improve naturally, significant DRA often persists indefinitely without treatment, with pathological distances frequently remaining above normal values even six months after delivery.
First Few Weeks Postpartum
6–12 Weeks Postpartum
3–6 Months
When Surgery is Considered
While conservative treatment is the preferred first step, surgical intervention may be considered in specific circumstances:
Recover faster, move better, and feel stronger with expert physiotherapy. Our team is here to guide you every step of the way.

Physiotherapy treatment for Diastasis Recti Abdominis (DRA) is a specialized process that prioritizes restoring the structural integrity of the abdominal wall through targeted, functional rehabilitation.
Deep Core Activation Exercises
Strengthening the transversus abdominis (TA) is the primary focus of conservative treatment.
Pelvic Floor Strengthening
Rehabilitating the pelvic floor is highly integrated into DRA treatment, with 87% of surveyed specialists including it in their care plans.
Breathing Techniques
Proper breathing is fundamental to managing intra-abdominal pressure during exercise.
Postural Training
Restoring proper alignment is vital to reducing chronic stress on the abdominal wall.
Progressive Strengthening
Rehabilitation follows the principle of progressive overload, carefully advancing as muscle control improves.
Preventing the worsening or recurrence of Diastasis Recti Abdominis (DRA) requires a proactive approach centered on managing intra-abdominal pressure and restoring the functional integrity of the core. According to the sources, the following strategies are essential for long-term recovery:
Practicing Proper Core Engagement
The foundation of prevention is the strengthening of the transversus abdominis (TA) muscle in isolation and during functional activities.
Monitoring for Abdominal "Doming"
Individuals must be vigilant for any visible bulging or doming along the midline of the abdomen during exercise or daily tasks.
Utilizing Safe Movement Mechanics
Education on proper body mechanics is vital for reducing daily strain on the abdominal wall.
Gradual Progression and Selective Exercise
A progressive overload principle must be followed to rebuild strength without causing recurrence.
Lifelong Commitment to Core and Pelvic Health
Long-term recovery and prevention are supported by a holistic approach to the "core" system.
Comprehensive Core and Abdominal Assessment
A thorough evaluation is necessary because DRA often goes undiagnosed and patients are frequently referred for other conditions, such as low back pain (80.7% of cases), pelvic floor dysfunction, or urinary incontinence,.
Targeted Deep Core Strengthening Exercises
Rehabilitation prioritizes the transversus abdominis (TA) muscle, as it can be trained to generate the force needed to resist the separation of the rectus muscles,,.
Pelvic Floor Rehabilitation
Pelvic floor training (Kegel exercises) is integrated into 87% of specialized care plans because of the high correlation between abdominal separation and pelvic health,.
Education on Safe Movement and Exercise
Education is stressed to ensure that daily activities do not hinder the healing of the linea alba (the connective tissue between the muscles),.
Gradual Progression Toward Physical Activity
Rehabilitation follows the principle of progressive overload, ensuring that the abdominal wall can handle increasing internal pressure without doming,.
Don't let diastasis recti limit your activities or affect your daily life. Our experienced team is ready to help you build a strong foundation for lasting recovery.
Book Your Specialized Assessment Today:
Phone: 905-669-1221
Location: 398 Steeles Ave W #201, Thornhill, ON L4J 6X3
Online Booking: www.vaughanphysiotherapy.com
Serving communities across Thornhill, Langstaff, Newtonbrook, Willowdale, North York, Markham, Richmond Hill, Concord, and North Toronto.
Conveniently located in the heart of Thornhill, offering flexible scheduling to accommodate your recovery needs.
Created by Sara Lam
Explore the latest articles written by our clinicians
.webp)
.webp)
.webp)


.avif)




