
Musculoskeletal or neurological condition affecting mobility or function.
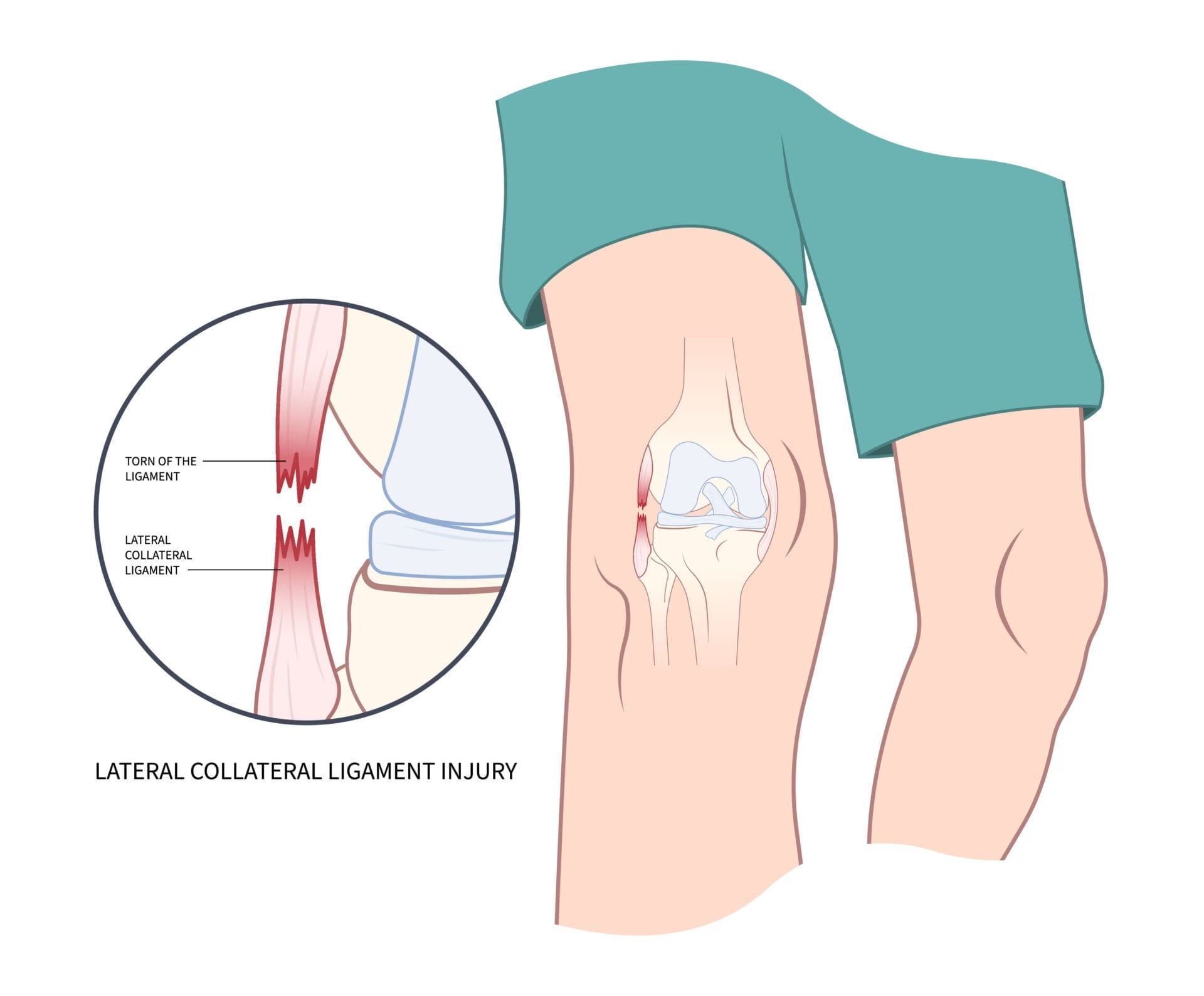
The Lateral Collateral Ligament (LCL) is a key knee ligament frequently described as a thin, cord-like structure. It originates from the lateral femoral condyle, specifically in a "saddle" located proximal and posterior to the lateral epicondyle. From its origin, it courses distally to insert on the lateral aspect of the fibular head, attaching anterior to the fibular styloid. These injuries typically occur due to direct contact, such as a blow to the medial side of the knee, or non-contact mechanisms like hyperextension stress.
Function and Role in Stability (Resists Varus Stress)
The LCL serves as the primary restraint to varus stress across all angles of knee flexion. It is most effectively evaluated by clinicians at 30° of flexion, the specific angle at which the maximum amount of varus laxity is observed after an injury. Beyond varus stability, the LCL acts as a secondary restraint to external rotation and posterior displacement of the tibia. It also works in conjunction with the Anterior Cruciate Ligament (ACL) to provide a secondary check against anterior tibial displacement. If the LCL is involved in an injury, the resulting instability is characterized by varus laxity, and patients often report a dull pain or a feeling of the knee "giving way" during activities.
LCL Injury Prevalence
Isolated LCL injury of the knee is a rare diagnosis, occurring in less than 2% of all athletic knee injuries. It is more commonly found in conjunction with other complex knee pathologies, particularly injuries to the posterolateral corner (PLC) or the cruciate ligaments (ACL and PCL). These injuries typically result from forces involving varus stress, external rotation, and hyperextension, which can occur through direct contact (such as a blow to the medial side of the knee) or non-contact mechanisms. While LCL injuries can occur in any sport, they are most frequently seen in soccer, tennis, and gymnastics, as well as in high-energy trauma like road traffic accidents, which accounted for over 50% of cases in some clinical reviews
Common Symptoms (LCL Sprain/Tear)
Following an LCL injury, patients may experience various functional impairments and clinical signs. Subjectively, patients often report a dull pain and a sensation of the knee "giving way" or instability, especially during "cutting" activities. Specific clinical signs observed include:
During physical examination, the figure-of-4 position is often used to tension and palpate the ligament to assess its integrity. Additionally, clinicians must evaluate the posterolateral corner using specific tests like the dial test, posterolateral drawer test, and recurvatum test to ensure a comprehensive diagnosis
Physiotherapy is critical for the rehabilitation of Lateral Collateral Ligament (LCL) injuries because early recognition and managed mobilization are vital to preventing chronic knee instability and the potential failure of other ligament repairs, such as the ACL. While isolated LCL injuries are rare, occurring in less than 2% of athletic knee injuries, Grade I and II tears are frequently managed non-surgically with a focus on early mobilization to achieve a favorable functional outcome
Addressing Impairments and Symptoms
The primary goal of rehabilitation is to address the functional limitations caused by the injury and restore the knee's natural kinematics and stability.
The prognosis and recovery timeline for a Lateral Collateral Ligament (LCL) injury depend significantly on the grade of the injury (severity), the presence of concomitant injuries to other knee structures, and the timing of the intervention. Because isolated LCL injuries are rare—occurring in less than 2% of athletic knee injuries—they are frequently diagnosed as part of more serious complex/multiligamentous ruptures involving the ACL, PCL, or posterolateral corner (PLC).
Recovery Expectations Based on Injury Grade
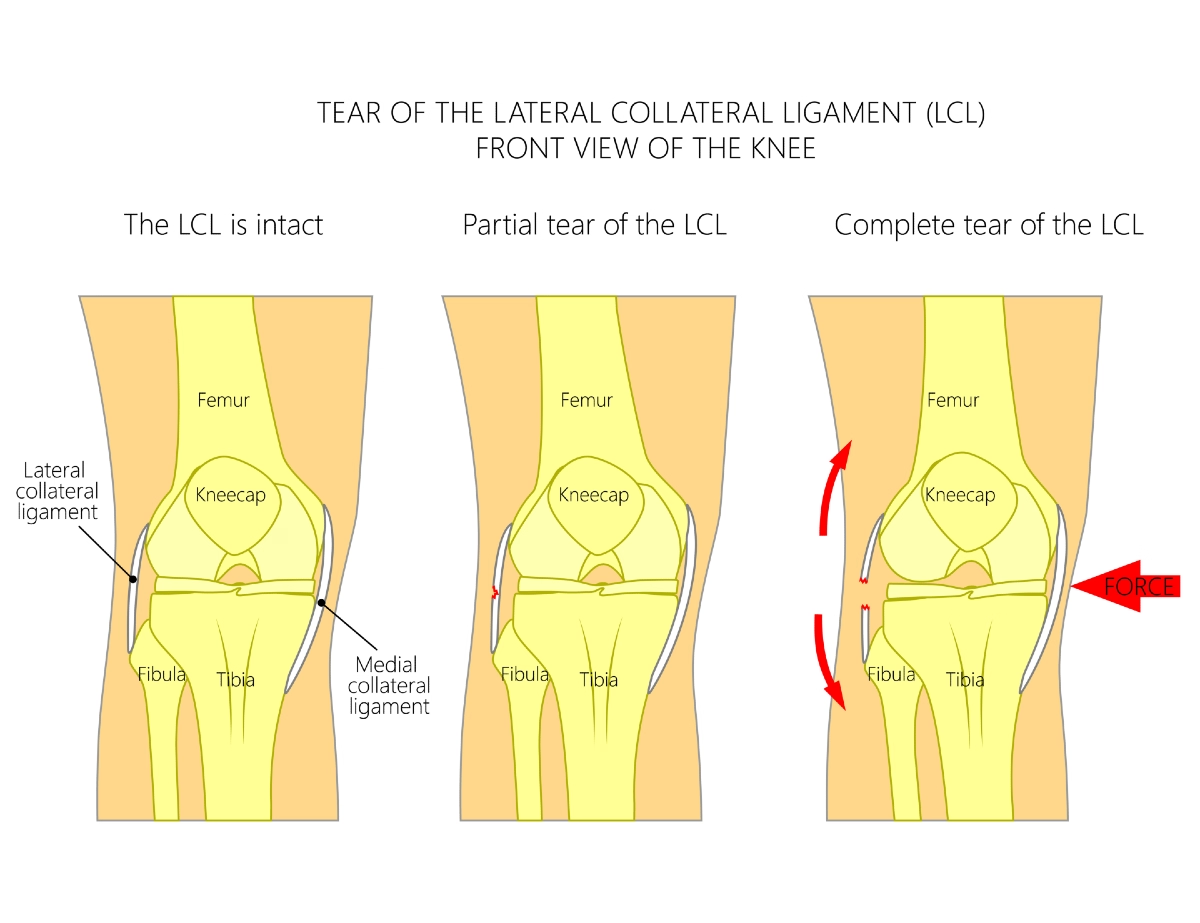
For isolated LCL injuries, treatment and recovery paths are typically guided by the following severity classifications based on MRI and physical examination:
Note on Professional Athletes: A study of National Football League (NFL) players with isolated Grade III LCL injuries found that those managed non-surgically were as likely to return to professional play as those who underwent surgery, and they did so more quickly. However, the sources note these results remain controversial, and many clinicians still advocate for surgical treatment of most Grade III injuries to prevent chronic instability.
Recovery in Combined/Complex Injuries (Surgical Cases)
When an LCL injury is part of a complex, multiligamentous injury, the recovery process is more intensive:
Failure to properly address LCL or PLC instability in complex cases can lead to chronic knee instability and the failure of other ligament repairs, such as the ACL
Factors Affecting Healing and Return to Activity
1. Injury Severity and Surgical Intervention
The most significant factor influencing recovery is the nature of the ligament injury and whether it occurs in isolation. Isolated Grade I and II tears can typically be managed non-surgically with early mobilization, often leading to full stability. However, the LCL is known to have unreliable healing compared to other ligaments like the MCL, leading many to advocate for a lower threshold for surgical intervention.
For Grade III injuries, non-operative results are often poor in general populations. While some professional athletes have returned to play quickly without surgery, surgical reconstruction is generally preferred over primary repair due to significantly lower failure rates (9% vs. 37%). In complex or multiligamentous cases, early operative treatment (ideally within the first 3 weeks) is vital to restore stability and prevent the failure of other ligament repairs, such as the ACL.
2. Rarity of Isolated Injuries and Trauma Mechanism
The mechanism of injury and the presence of concomitant damage are critical. Isolated LCL injuries are extremely rare, occurring in less than 2% of athletic knee injuries. Most high-grade LCL injuries are part of serious combined ruptures involving the ACL, PCL, or the posterolateral corner (PLC). These are often caused by high-energy trauma, with traffic accidents accounting for 52% of cases in some clinical reviews. The presence of sagittal instability (from cruciate damage) directly influences varus instability and complicates the recovery process.
3. Adherence and Individual Progression
Progression in rehabilitation is increasingly influenced by the use of anatomic reconstruction techniques. These procedures are designed to restore physiologic forces on the graft, which allows for early range of motion during the rehabilitation phase.
4. Achieving Milestones (Return to Activity Expectations)
In mild cases (Grade I instability), early mobilization has been shown to result in complete stability at long-term follow-up. For more severe or surgically treated injuries, milestones are centered on restoring physiologic knee anatomy and kinematics.
Recover faster, move better, and feel stronger with expert physiotherapy. Our team is here to guide you every step of the way.

The following guidelines are derived from recent clinical reviews and biomechanical studies. They emphasize that while isolated Grade I and II LCL injuries often succeed with non-operative early mobilization, Grade III or complex injuries typically require anatomic reconstruction to allow for a more aggressive, staged approach to physical therapy.
Physiotherapy Treatment Approaches for LCL Injuries
1. Initial Protection and Motion Restoration (Weeks 0–6)
The primary goals of this stage are to promote tissue healing, reduce initial impairments like pain and swelling, and restore knee extension. Because the LCL has unreliable healing compared to other knee ligaments, protection of the healing fibers or surgical graft is paramount. Modern anatomic reconstructions are designed to restore physiologic forces, which uniquely allows for early range of motion (ROM) during this phase.
◦ Anatomical Considerations: The LCL is maximally separated (taut) in full extension and progressively slackens as the knee flexes, reaching approximately 88% of its extended length at 130° of flexion.
◦ Kinematic Shifts: Physiotherapists must respect the shifting orientation of the ligament, which moves from an 11° posterior slope in extension to a 19° anterior slope in deep flexion.
◦ Flexion Management: While the LCL slackens during flexion, allowing for natural tibial rotation, clinicians should be aware that internal rotation beyond 15° can separate the attachment sites and increase tension, particularly between 60° and 105° of flexion.
◦ Biceps Femoris Synergy: Rehabilitation should specifically target the biceps femoris (both long and short heads). This muscle acts as a dynamic controller of the LCL; its contraction creates a "bowstring effect" that stabilizes the lateral compartment.
◦ Quadriceps Control: Restoring quadriceps function is essential to prevent a flexed-knee gait, though specific use of high-intensity electrical stimulation is noted in general clinical practice to combat inhibition.
2. Controlled Strengthening and Gait Training (Weeks 4–12)
Once initial healing has occurred, the focus shifts to full weightbearing and developing muscular strength. For patients who underwent anatomic reconstruction, this phase is supported by the surgical technique's ability to restore physiologic forces, which allows for early range of motion during rehabilitation.
◦ Influence of Rotation: Movement patterns should be carefully monitored because internal tibial rotation significantly influences ligament tension. Between 60° and 105° of flexion, internal rotation can cause the LCL attachment sites to separate to greater than 100% of their length in full extension, potentially placing distraction stress on a healing ligament or graft. Conversely, external rotation beyond 30° causes the sites to approximate rapidly, making the ligament appear visually and palpably slack.
3. Neuromuscular Control and Low-Impact Conditioning (Months 3–6)
In the later stages of recovery, the program integrates activities to improve dynamic stability and restore previous levels of performance.
◦ Professional Athletes: In elite populations like NFL players, those with isolated Grade III injuries managed non-surgically have returned to play more quickly than those managed surgically, though this remains a controversial management path.
◦ General Outcomes: Patients typically report marked improvements in pain, stiffness, and subjective functional scores by 2 years following anatomic LCL reconstruction.
4. Sport Preparation and High-Level Agility (Months 6–9+)
Based on clinical sources, there are clinical milestones, biomechanical constraints, and long-term outcome data that define readiness for high-level activity and sport-specific movements.
5. Long-Term Maintenance and Prognosis (2+ Years)
Long-term maintenance is focused on preserving joint kinematics and preventing the failure of concurrent repairs, such as the ACL or PCL.
Biomechanical Precision and Surgical Accuracy
Clinical sources emphasize that long-term knee health is fundamentally tied to the precise restoration of physiologic anatomy. Inaccurate reconstruction—specifically the "nonanatomic" placement of a graft—is a leading cause of failure and can disrupt the normal dynamics of knee motion, potentially resulting in "premature arthritic changes". For instance, placing a femoral attachment too far anteriorly can cause undue tension during extension, while a posterior placement leads to rapid slackening during flexion. Successful management requires the reconstructive surgeon to precisely reproduce the positioning and functioning of the natural LCL to restore the knee to its previous level of performance
Dynamic Control and Stabilization
A critical factor in preventing re-injury is the "dynamic control" exerted by the biceps femoris (both long and short heads). During activity, the contraction of these muscle fibers creates a "bowstring effect" on the LCL, providing essential dynamic stabilization to the lateral compartment. Rehabilitation must ensure these dynamic stabilizers are fully functional to complement the static restraints and maintain the knee's rotational and varus stability.
Addressing Gait Mechanics and Varus Stress
The sources highlight that the knee is subject to the greatest force during gait, particularly during the stance phase. At this point, physiological varus angulation reaches its maximum as the knee enters full extension, putting significant stretch on the lateral structures. Because the LCL is the primary restraint to varus rotation at all positions of flexion, long-term health depends on the ligament's ability to withstand these repetitive loads during the gait cycle.
Early Recognition to Prevent Secondary Failure
Preventing chronic instability requires the "early recognition" and management of LCL and posterolateral corner (PLC) injuries. The sources warn that "clinically unrecognized posterolateral injuries" are a frequent cause of chronic knee instability and the subsequent "post-surgical failure of the cruciate ligaments" (ACL or PCL). For high-grade injuries (Grade 2+ or 3+ instability), "early operative treatment"—ideally performed within the first three weeks of injury—is recommended to provide the most favorable long-term stability and functional outcomes.
Note on Footwear and Orthotics: The provided sources focus primarily on surgical techniques, anatomy, and clinical evaluation; they do not provide specific data or recommendations regarding the use of footwear or orthotics for preventing LCL sprains or correcting varus mechanics. Would you like me to create a tailored report summarizing the biomechanical restraints of the LCL or perhaps a quiz on the clinical evaluation of lateral knee injuries?
Training Modifications & Load Management
Long-term prevention of LCL recurrence is achieved by establishing dynamic stability and restoring precise physiologic anatomy, which allows the knee to withstand the significant forces applied during functional activities, particularly the stance phase of gait.
Dynamic Stability and Strength Maintenance: The most critical long-term factor for joint health is maintaining and improving the knee's dynamic stability through the following mechanisms:
Load Management and Activity Progression:
The progression of rehabilitation must be tailored to the biomechanical behavior of the ligament and the type of surgical intervention used.
Our Specialized Approach to Rehab
Our comprehensive treatment programs include:
Why Choose Our Clinic for LCL Treatment?
Evidence-Based Expertise
Personalized Care
Comprehensive Recovery Support
Don’t let an LCL injury hold you back. At Vaughan Physiotherapy Clinic, our clinicians specialize in ligament rehabilitation, knee stability training, and post-operative LCL/PLC protocols. We help athletes, workers, and everyday movers get back to confident, pain-free activity.
Whether your goal is walking without pain, returning to sport, or preventing re-injury, our team will design a personalized, evidence-based LCL rehab program tailored to your stage of healing.
Book Your Specialized LCL Assessment Today:
Serving Thornhill, Langstaff, Newtonbrook, Willowdale, North York, Markham, Richmond Hill, Concord, and North Toronto. Evening and weekend appointments available.
Created by Sara Lam
Explore the latest articles written by our clinicians
.webp)
.webp)
.webp)


.avif)




