What Is Lumbar Instability? Understanding the Condition
Lumbar segmental instability is a condition where the stabilizing systems of the spine fail to maintain the intervertebral neutral zone—the region of laxity around a spinal segment's neutral position—within physiological limits. This failure results in excessive or erratic intersegmental motion, which can lead to incapacitating pain, deformity, or functional disability.
Conceptual Framework
There are two primary types of instability:
Mechanical (Radiological) Instability: Identified via imaging (like flexion-extension X-rays) as excessive translational or angular movement, such as a sagittal translation larger than 3 mm.
Functional (Clinical) Instability: Characterized by a lack of neuromuscular control of the vertebral segments during activities, even if radiological findings are normal. Functional instability is often viewed as a "movement control problem" within the neutral zone.
The Three Stabilizing Subsystems
Stability is maintained by the interdependent interaction of three systems:
The Passive Subsystem: Consists of the vertebrae, intervertebral discs, facet joints, and ligaments. These structures provide resistance mainly at the end of a movement.
The Active Subsystem: Composed of muscles and tendons. The local muscle system (e.g., multifidus, transversus abdominis) is responsible for providing segmental stability and controlling individual vertebrae, particularly in the neutral zone.
The Neuromuscular Subsystem: The nerves and central nervous system that coordinate muscle activity. Instability often arises from impaired motor control, such as delayed muscle response times or faulty recruitment patterns in the deep stabilizers.
Common Symptoms and Clinical Presentation
Patients with lumbar instability frequently report:
Fluctuating Pain: Chronic and recurrent low back pain described as "constant" (55%) or "recurrent" (70%).
Sudden Movement Alterations: Feelings of the back "giving way" (20%), "catching" (45%), or "locking" (20%).
Painful Transitions: Aggravation during transitional movements like sitting-to-standing, bending, lifting, or rotating.
Postural Vulnerability: Difficulty with unsupported sitting or pain that worsens with sustained positions.
Aberrant Movement Patterns: During physical examination, patients may display a painful arc during flexion, sudden "hitching" or "shaking," or the need to use their hands to "climb" up their thighs to return to an erect position (Gower sign).
Relief with Stability: A significant reduction in pain is often noted when the deep abdominal muscles are activated during provocative movements.
Normal Neurological Tests: Unless other pathologies are present, neurological examinations and neural tissue provocation tests are generally normal.
Prevalence and Associated Factors
Lumbar instability as a significant subgroup within the chronic low back pain population.
Demographics: It is commonly observed in patients with chronic back pain, particularly those between ages 20–60.
Risk Factors: Instability is frequently associated with spondylolisthesis (where one vertebra slips over another) and spondylolysis. It can develop suddenly from a single event injury or gradually due to multiple minor traumas.
Conditioning: Impaired segmental stability is linked to muscle dysfunction, specifically atrophy or reduced endurance of the multifidus and transversus abdominis
Anatomy of the Low Back (Relevant to Instability)
The Passive SubsystemThis system provides structural integrity and is the primary restraint at the end of a range of movement. Components include:
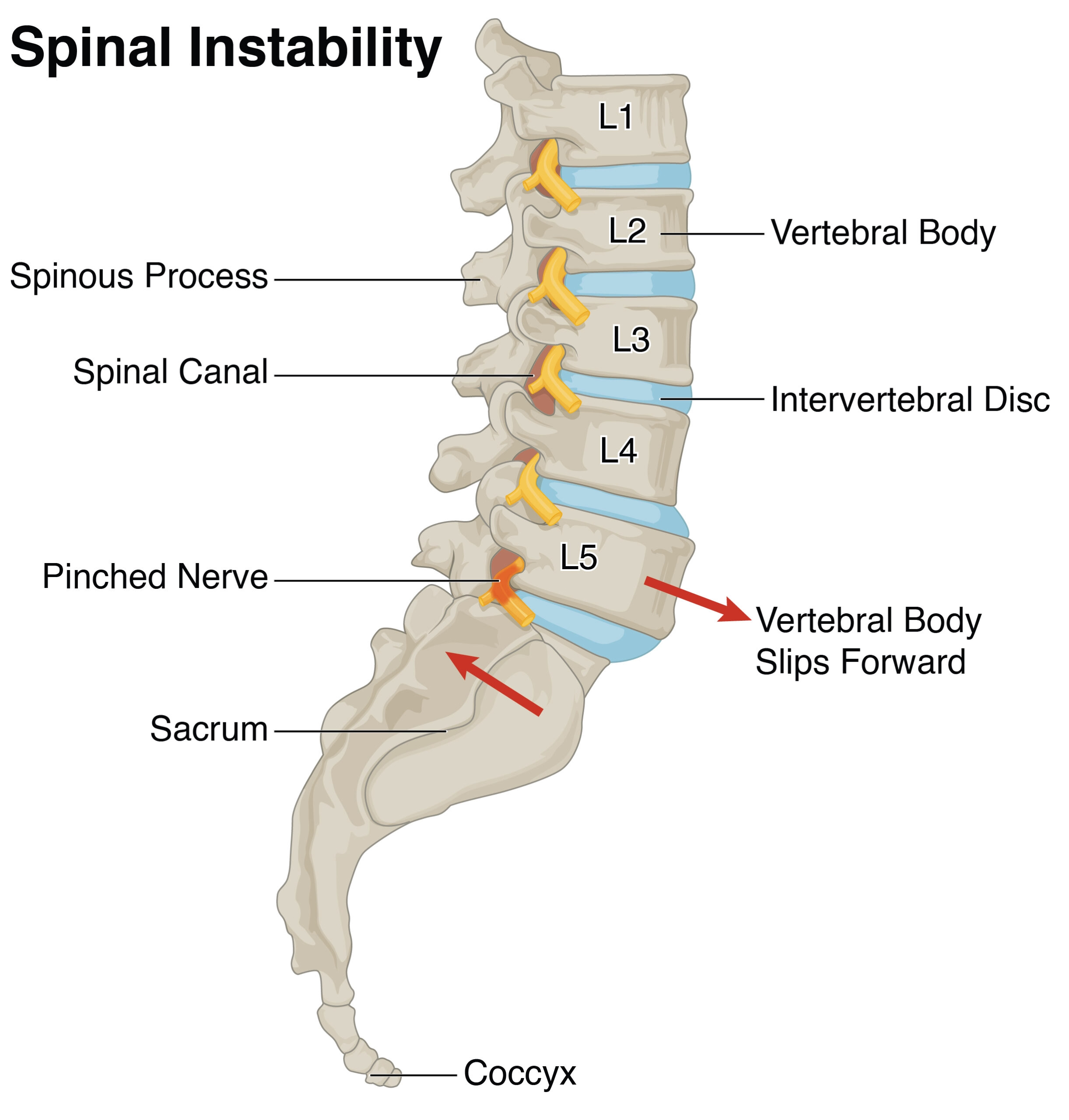
Vertebrae and Facet Joints (L1–L5)
Features: The vertebrae are 5 bones within the lower spine that are designed to withstand high compressive force which each have a:
Vertebral body - responsible for weight bearing
Facet joints - guides motion
Spinous and transverse processes - areas for muscles to attach to
Sacrum
The sacrum is a bony structure located at the base of the spine, serving as the foundation of the lumbosacral region.
Key functional and anatomical points regarding the sacrum include:
Lumbosacral Junction: The area where the last lumbar vertebra (L5) meets the first segment of the sacrum (S1) is known as the L5-S1 level. This junction is a frequent site for mechanical issues like disk herniations.
Nerve Roots: The S1 nerve root exits in this region; compression of this root can lead to pain, loss of reflexes, or sensory changes in the lower limbs.
Load Transmission: The sacroiliac joints connect the sacrum to the pelvis, helping to transfer mechanical loads between the spine and the lower limbs.
Lumbosacral Musculature: The muscles surrounding this area, often referred to as the lumbosacral musculature, are frequently involved in strains and spasms associated with mechanical low back pain
Intervertebral Discs
Located between each vertebrae
Each disc has:
Annulus fibrosis - tough fibrous outer layer
Nucleus pulposis - gel-like center
Roles of the discs include shock absorption, movement, and load transmission
Muscles and Ligaments
Core Spinal Stabilizers: The transversus abdominis is identified as a primary core stabilizer of the spine. The multifidus is also a key muscle involved in maintaining segmental stability.
Trunk and Back Extensor Muscles: These provide the force-generating capacity and endurance necessary for the back to sustain normal daily activities and maintain posture.
Abdominal Muscles: These work in coordination with the back extensors to ensure lumbar stability.
Hamstrings: Although located in the thighs, this muscle group is functionally linked to the low back; their flexibility supports the overall range of motion for the lumbar region
The Active SubsystemThe active system is responsible for providing dynamic stability, particularly within the neutral zone where the passive system is less effective.
Local Muscle System (Segmental Stabilizers): These muscles attach directly to the vertebrae and are responsible for controlling individual segments. Key muscles include the multifidus (which provides two-thirds of active stiffness at L4–L5), transversus abdominis (the "muscular corset"), diaphragm, and the pelvic floor.
Global Muscle System (Prime Movers): Large torque-producing muscles like the rectus abdominis and external obliques act on the trunk to provide general stabilization and movement but have less direct influence on individual segments.
Mechanism of Stability: Stability is achieved through antagonistic co-activation (muscles working together to stiffen the spine) and increased intra-abdominal pressure (created by the coordinated contraction of the diaphragm, transversus abdominis, and pelvic floor).
The Neural Control SubsystemThis is the most complex system, acting as the "coordinator" for the active system.
Function: It computes data from proprioceptive receptors located in both the passive and active structures to determine the necessary level of muscle activation for various tasks.
How Does Lumbar Instability Develop? Causes and Risk Factors
Lumbar instability typically develops when there is a breakdown in the interdependence of the three subsystems that stabilize the spine: the passive subsystem (vertebrae, discs, ligaments), the active subsystem (muscles and tendons), and the neural control subsystem (nerves and coordination)
Common causes:
Injury and Trauma: Clinical data shows a split in how instability begins: 50% of patients develop it following a single-event traumatic injury (such as a fall), while the other 50% develop it gradually through multiple minor traumatic incidents.
Repetitive Loading: Cumulative stress from repetitive bending, twisting, or rotation—particularly in flexion or extension—renders the spine's "neutral zone" (the area where the spine has minimal resistance to motion) biomechanically vulnerable.
Disc Degeneration: As intervertebral discs degenerate and lose height, the passive restraint of the spinal segments decreases. While mild to moderate degeneration often results in erratic motion and increased neutral zone size, severe "Grade V" degeneration may actually lead to "restabilization" as the body forms osteophytes to compensate for the instability.
Bony Defects: Conditions like spondylolysis (stress fractures) and spondylolisthesis (slippage of vertebrae) are primary structural causes that lead to excessive intersegmental motion
Risk factors:
Muscle Atrophy and Dysfunction: The multifidus is a critical stabilizer, providing two-thirds of the stiffness at the L4–L5 level. Studies show that multifidus atrophy occurs rapidly after a back injury and does not recover automatically even after the pain resolves, creating a high risk for recurrent instability.
Delayed Neuromuscular Control: A major risk factor is the delayed activation of the transversus abdominis. In healthy individuals, this muscle activates before limb movement to stabilize the spine; in those with back pain, this anticipated automatic response is significantly slowed.
Hypermobility and Ligament Laxity: While hypermobility (excessive range of motion) is not the same as instability, joints that are hypermobile generally have a higher tendency toward clinical instability due to the increased demand on the muscular system to control that extra range.
High-Demand Physical Activity: Specific movement patterns are linked to certain activities. For example, the "Extension Pattern" of instability is common in sports involving frequent extension and rotation, such as throwing or fast running.
Compensatory Muscle Substitution: When deep stabilizers (local muscle system) fail, the body may attempt to compensate by over-activating global muscles like the rectus abdominis or erector spinae. This "bracing" strategy is often sub-optimal and can lead to increased pain and muscle fatigue
Why Physiotherapy Is Critical for Lumbar Instability Recovery
Physiotherapy targets the primary dysfunction behind lumbar instability: impaired motor control and reduced dynamic stability.
Key benefits of physiotherapy include:
Muscle Atrophy and Dysfunction: The multifidus is a critical stabilizer, providing two-thirds of the stiffness at the L4–L5 level. Studies show that multifidus atrophy occurs rapidly after a back injury and does not recover automatically even after the pain resolves, creating a high risk for recurrent instability.
Delayed Neuromuscular Control: A major risk factor is the delayed activation of the transversus abdominis. In healthy individuals, this muscle activates before limb movement to stabilize the spine; in those with back pain, this anticipated automatic response is significantly slowed.
Hypermobility and Ligament Laxity: While hypermobility (excessive range of motion) is not the same as instability, joints that are hypermobile generally have a higher tendency toward clinical instability due to the increased demand on the muscular system to control that extra range.
High-Demand Physical Activity: Specific movement patterns are linked to certain activities. For example, the "Extension Pattern" of instability is common in sports involving frequent extension and rotation, such as throwing or fast running.
Compensatory Muscle Substitution: When deep stabilizers (local muscle system) fail, the body may attempt to compensate by over-activating global muscles like the rectus abdominis or erector spinae. This "bracing" strategy is often sub-optimal and can lead to increased pain and muscle fatigue
What to Expect: Prognosis and Recovery Timeline
Recovery is a progressive process divided into cognitive, associative, and autonomous stages of learning.
3–6 Weeks (Initial Control): In this "cognitive stage," the primary focus is on a high level of awareness to isolate the co-contraction of the local muscle system (specifically the transversus abdominis and multifidus) without substituting with global muscles. Patients can expect to achieve a degree of pain control in static postures (sitting and standing) during this period.
8 Weeks to 4 Months (Refinement and Strength): During the "associative stage," patients refine movement patterns by breaking down faulty, pain-provocative motions (like bending or lifting) into component parts and repeating them with high frequency (50–60 times). Successful 10-week clinical trials have demonstrated significant reductions in pain and disability by this stage. Patients typically report the ability to perform previously aggravating activities without pain as the motor patterns begin to become automatic.
Beyond 4–6 Months (Automaticity and Long-Term Stability): The goal is the "autonomous stage," where the spine is dynamically stabilized automatically during the functional demands of daily living. Long-term data (including 30-month follow-ups) show that patients who successfully reach this stage maintain their improvements in pain and function.
Factors Influencing Success
Adherence and Maintenance: For long-term prevention of relapses, patients must maintain local muscle system control functionally through ongoing postural awareness and regular general exercise.
Condition Severity: Patients with high levels of irritability who cannot tolerate compressive loading in any position may have a poor prognosis for conservative management.
Compliance: The success of the intervention is heavily influenced by the patient's level of compliance and the skill of the therapist in identifying specific motor control dysfunctions.
Predictors of Success: Clinical research identifies several factors that predict a positive response to stabilization programs, including an age lower than 40, a positive prone instability test, and the presence of aberrant movement patterns.
Start Your Journey to
Better Health Today
Recover faster, move better, and feel stronger with expert physiotherapy. Our team is here to guide you every step of the way.
Motor Control Training Sources categorize this as the Cognitive Stage, requiring high awareness to isolate the co-contraction of the transversus abdominis and multifidus without substitution from global muscles like the rectus abdominis.
Isolation: Training begins with low-load (1–3% of maximal contraction) isometric contractions, often using the "hollowing" or "abdominal drawing-in" maneuver to facilitate the deep stabilizers.
Precision: These exercises are performed with controlled respiration and a focus on maintaining a neutral lordosis.
Progression: Once isolation is achieved (typically taking 3–6 weeks), the patient moves into functional tasks.
Core Strengthening While "core strengthening" is often used broadly, the sources distinguish between training for stiffness/stability and traditional strength.
Recommended Exercises: The sources explicitly support isometric horizontal side supports (side planks) to challenge the lateral obliques and quadratus lumborum, and quadruped leg extension with contralateral arm raising (bird-dogs).
Load Management: Clinicians are cautioned that certain traditional exercises, such as full trunk extensions, can impose high compressive and shear loads that may be deleterious for patients with instability.
Movement Retraining This represents the Associative Stage of recovery, where faulty movement patterns are identified and broken down into components for high-repetition retraining (50–60 repetitions).
Pattern-Specific Retraining: Therapy is tailored to the patient’s directional pattern, such as retraining sit-to-stand or lifting without the "hinging" or "catching" characteristic of instability.
Reducing Compensations: A primary goal is to inhibit the sub-optimal strategy of "bracing" with global muscles during low-load tasks, which patients often do in an attempt to preserve stability.
Manual Therapy (Adjunct) Manual therapy is used primarily as a diagnostic tool and a secondary treatment aid.
Joint Mobilization: Techniques like PA (posteroanterior) glides are used to identify hypermobile segments and assess local stiffness.
Soft-Tissue Release:Muscle release techniques are recommended to inhibit overactive global muscles (like the erector spinae) that may be compensating for weak deep stabilizers.
Functional and Sport-Specific Conditioning This final stage, the Autonomous Stage, aims for the spine to be dynamically stabilized automatically during daily living.
Return to Activity: Patients are encouraged to engage in regular aerobic exercise, such as walking, while maintaining postural awareness and low-level stabilizer co-contraction.
Kinetic Chain: While the sources focus heavily on the lumbar spine, they acknowledge the role of the diaphragm and pelvic floor in creating intra-abdominal pressure to support the lumbosacral region.
Education Education is considered a "logical management strategy" to ensure long-term compliance and prevention.
Posture and Ergonomics: Patients are taught proper mechanics for sitting, standing, and lifting to avoid prolonged postural stresses that increase the "neutral zone" of laxity.
Flare-up Management: Education focuses on identifying aggravating movement quadrants and using active stabilizer activation as a form of pain control during transitional activities
Preventing Lumbar Instability Recurrence
Maintain a Regular Core Stability Program Sources define a successful core program not just by muscle size, but by the ability to stabilize the "neutral zone"—the region of laxity where the spine is most vulnerable to erratic motion.
Target the Local Muscle System (LMS): You must focus on the deep stabilizers that attach directly to the vertebrae, specifically the multifidus, transversus abdominis (TrA), and the pelvic floor.
Automaticity: The goal of a regular program is to reach the "autonomous stage" of motor learning, where these muscles dynamically stabilize the spine automatically during the functional demands of daily life.
Endurance over Strength: Because these muscles must work continuously to maintain stability, they require low-load endurance training (as low as 1–3% of maximal contraction) rather than high-intensity strength training.
Avoid Prolonged Poor Postures Prolonged postures can cause mechanical fatigue or deformation of the soft tissues, increasing the neutral zone of laxity.
Directional Sensitivity: Identifying your specific pattern is key. For example, those with a "flexion pattern" often have a loss of segmental lordosis and struggle with semi-flexed or slouched sitting, while those with an "extension pattern" may hyperlordose (arch) the spine during standing or overhead activities.
Segmental Control: Maintenance involves training the ability to differentiate pelvic and low lumbar movement from the thoracic spine and hips to maintain a neutral lordosis.
Use Proper Lifting Mechanics Lifting imposes significant shear and compressive forces that the passive system (ligaments and discs) cannot handle alone.
Intra-Abdominal Pressure (IAP): Proper mechanics utilize the "muscular corset" (TrA, obliques, diaphragm, and pelvic floor) to increase IAP. This provides a stiffening effect that constrains spinal movement in all directions without requiring the erector spinae to produce high compressive loads.
Motor Control: Lifting should be retrained in the "associative stage" by breaking the movement into component parts and repeating them until the segmental control is smooth and controlled.
Strengthen Hips and Pelvis to Offload the Lumbar Spine Sources highlight that the lumbar spine does not work in isolation; the kinetic chain—specifically the hips and pelvis—plays a major role in stability.
Pelvic Interaction: The pelvic floor co-activates with the TrA, and its contraction is a primary strategy for facilitating deep spinal stability.
Lateral Stability: The quadratus lumborum is an essential lateral stabilizer, especially during heavy lifting and upright holding.
Psoas Major: This muscle attaches to the lumbar vertebrae and contributes to stability in the frontal and transverse planes.
Gradually Increase Training LoadsProgressive loading is necessary, but the sources caution against advancing too quickly.
Avoid Deleterious Loads: Certain common exercises, such as full trunk extensions or simultaneously lifting the upper body and legs in prone, can impose dangerously high compressive loads for an unstable segment.
The Motor Learning Progression: Start with low-load isolation in Stage 1 (Cognitive), progress to functional patterns in Stage 2 (Associative), and finally move to high-load or sport-specific tasks in Stage 3 (Autonomous).
Early Intervention if Symptoms Re-emergeBecause recurrence is a typical characteristic of mechanical back pain—with rates between 60% and 80%—early intervention is vital to prevent the condition from becoming chronic.
Muscle Recovery is Not Automatic: Research shows that the multifidus does not recover automatically after an episode of back pain, even after the pain disappears. Specific exercises are required to "wake up" these muscles to prevent future instability.
Diagnostic Precision: Re-emerging symptoms should be evaluated for "aberrant movements" (like an instability catch or painful arc) which indicate a loss of functional control that needs immediate motor retraining
Our Specialized Approach to Rehabilitation
Precise Assessment of Segmental Control Sources emphasize that effective management begins with an accurate clinical diagnosis, as conventional radiology is often insensitive to functional (clinical) instability.
Identifying Aberrant Motion: Clinicians look for "aberrant movement patterns" during trunk flexion and extension, such as an instability catch, a painful arc, or the Gower sign (climbing up the thighs with the hands to stand up).
Directional Specificity: Assessment aims to identify the specific "movement quadrant" where the spine is vulnerable—such as flexion, extension, or lateral shift patterns—to ensure the program is tailored to the patient's unique injury.
Manual Testing: Techniques like Passive Accessory Intervertebral Motion (PAIVM) tests are used to evaluate local hypermobility and stiffness at specific segmental levels.
Guided Activation of Deep StabilizersA core component of specialized rehab is "waking up" the local muscle system, which includes the multifidus and transversus abdominis (TrA).
The Role of Guidance: Because these muscles are deep and their contractions are subtle, guidance is essential. Manual palpation by a therapist is described as "crucial" to ensure the correct muscle is firing without "substitution" from larger global muscles like the rectus abdominis.
Visual Feedback: The use of ultrasound imaging is highlighted as a modern technique to provide real-time visual feedback, allowing patients to see their muscles contracting as they learn the "hollowing" or abdominal drawing-in maneuver.
Personalized, Progressive Motor-Control ProgramsResearch details a structured, three-stage motor learning model designed to move the patient from conscious isolation to automatic stability:
Stage 1: Cognitive (Isolation): Patients learn to isolate the co-contraction of the TrA and multifidus at very low loads (1–3% of maximal contraction) while maintaining a neutral lordosis and controlled breathing.
Stage 2: Associative (Refinement): Faulty and pain-provocative movement patterns are broken down into components and retrained with high repetitions (50–60 reps) to refine the quality of movement.
Stage 3: Autonomous (Automaticity): The final goal is for the stabilizers to activate automatically during the functional demands of daily life, requiring little to no conscious attention.
Integration into Functional and Sport-Specific TasksRehabilitation is not complete until the new motor skills are integrated into the patient's actual life and athletic requirements.
Functional Progression: Training progresses from static postures to dynamic tasks like sitting-to-standing, lifting, bending, and twisting.
Sport-Specific Loading: For athletes, the program addresses high-demand patterns, such as the extension/rotation forces seen in throwing, running, or swimming, ensuring the local muscle system can handle these specific stresses.
Education and Multidisciplinary CoordinationEducation is viewed as a logical management strategy for long-term self-management.
Self-Correction: Patients are educated on posture strategies and ergonomics to avoid prolonged mechanical stress on vulnerable segments.
Psychosocial Considerations: For chronic cases where pain is associated with psychosocial factors, the sources suggest that a multidisciplinary biopsychosocial approach—which may involve coordination with other health professionals—is more effective than physical treatment alone
FAQs
Is lumbar instability the same as hypermobility?
Not exactly.
Hypermobility is a quantitative measure, defined as an excessive range of motion at a joint based on a person's age and activity level.
In contrast, instability is a qualitative measure characterized by aberrant or erratic motion during movement, such as a "catch," "shake," or "hitch".
While they can coexist and a hypermobile joint may be more prone to instability, they are not systematically correlated; a person can have radiological hypermobility without the pain-inducing functional deficits of instability
Can lumbar instability be cured?
While research doesn't often use the word "cure," they provide strong evidence that patients can achieve long-term reductions in pain and functional disability.
Research into specific stabilizing exercise programs has shown that patients can maintain significant improvements in pain and quality of life for as long as 30 months follow-up after completing a 10-week intervention.
Success is highly dependent on patient compliance and the retraining of automatic muscle recruitment patterns
Do I need imaging?
Typically, no.
Conventional radiological testing, such as standard X-rays, is often insensitive and unreliable for accurately detecting the abnormal intersegmental motion associated with clinical instability.
Functional instability can cause significant pain even in the absence of any radiological anomaly. Consequently, diagnosis is best achieved through a clinical assessment of subjective complaints (like a feeling of "giving way") and objective signs (like "aberrant movement patterns" during trunk flexion)
Is a brace helpful?
Bracing may offer short-term symptomatic relief and can be a clinical indicator that a patient will respond well to a stabilization program.
However, it is not a replacement for motor control training.
While a brace provides passive support, the goal of physiotherapy is to reprogram the active muscle subsystem (such as the transversus abdominis and multifidus) to dynamically stabilize the spine automatically during daily tasks
Can I exercise with lumbar instability?
Yes—exercise is essential for management.
However, the focus must shift from general weight training to neuromuscular control and endurance.
The most effective approach involves a "motor learning model" that starts with low-load, high-precision isolation of the deep stabilizers before progressing to functional movements.
Proper technique is critical, as certain traditional exercises (like full trunk extensions) may impose high compressive or shear loads that could be deleterious
Take the First Step Toward Recovery
Don't let lumbar instability limit your activities or affect your daily life. Our experienced team is ready to help you build a strong foundation for lasting recovery.
Book Your Specialized Assessment Today:
Phone: 905-669-1221
Location: 398 Steeles Ave W #201, Thornhill, ON L4J 6X3


.webp)
.webp)
.webp)


.avif)




