What Is MCL Sprain Rehabilitation? Causes and Symptoms
The Medial Collateral Ligament (MCL) is a critical passive stabilizer of the knee, measuring approximately 8 to 10 cm in length. It originates on the medial femoral epicondyle and attaches distally to the tibia. An MCL sprain involves a stretch or tear of this ligament, which is the most common ligamentous injury of the knee, particularly prevalent in sports like football. Unlike some other ligaments, the MCL has a good self-healing capacity due to its high vascularization and relationship to the joint capsule
Symptoms of MCL Sprains:
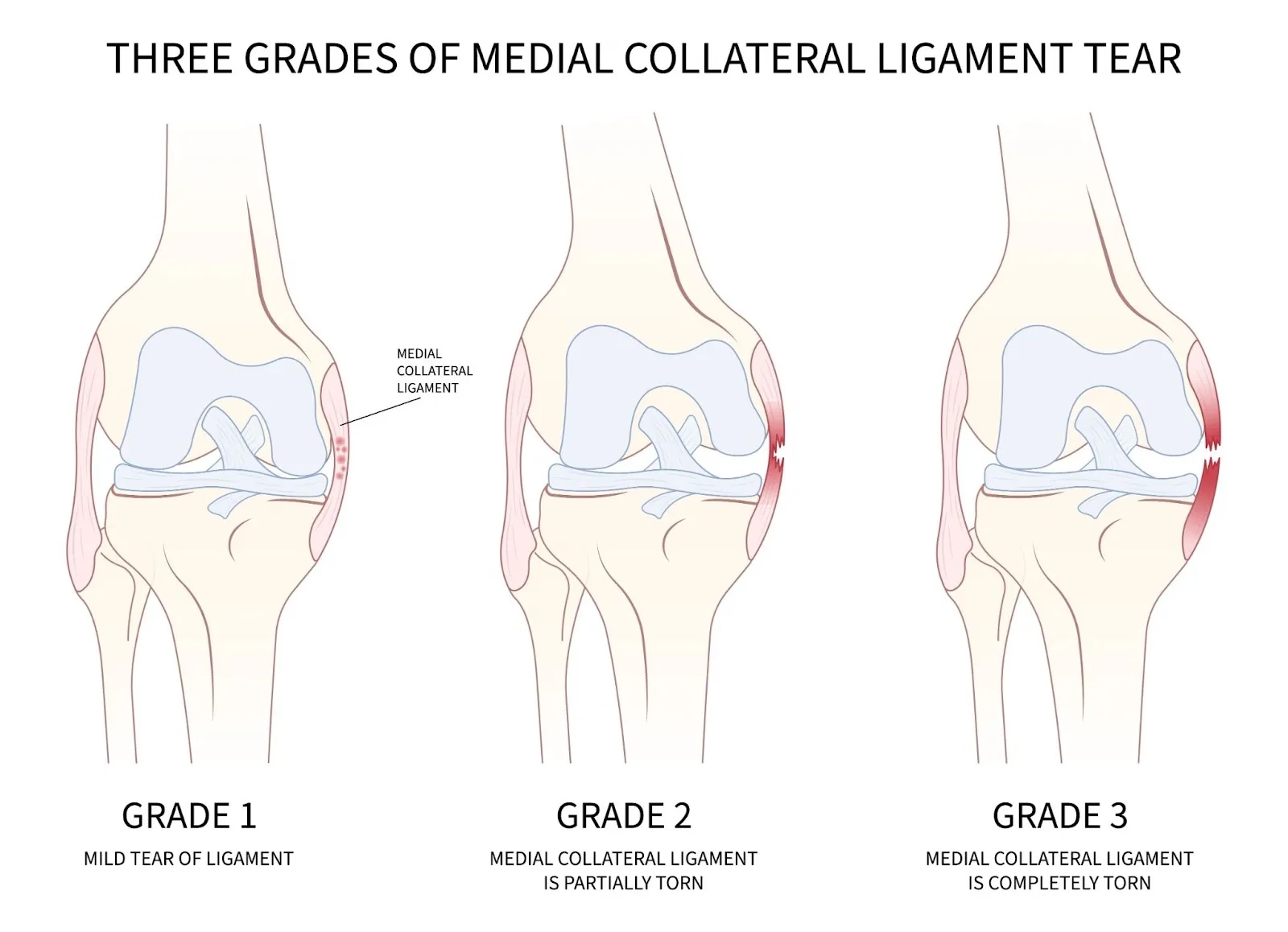
The symptoms of a Medial Collateral Ligament (MCL) sprain are primarily categorized by the severity of the injury, which is classified into three grades based on the extent of ligamentous disruption and joint laxity.
Symptoms by Injury Grade
Grade I (Mild): This involves a minimal number of torn fibers. The primary symptoms are localized tenderness and pain on the medial (inner) side of the knee, but there is no demonstrable instability or valgus laxity.
Grade II (Moderate): This is a partial tear with greater fiber disruption. Symptoms include localized pain and slight to moderate abnormal motion (a medial joint opening of 6–10 mm). A defining clinical symptom is that a firm end point is still felt when the knee is subjected to valgus stress.
Grade III (Severe): This represents a complete tear of the ligament. It is characterized by significant joint instability and a medial joint opening of greater than 10 mm. Clinically, there is no palpable end point when testing for stability.
Physical and Clinical Impairments
Beyond the grading system, the sources identify several common impairments associated with MCL injuries:
Pain and Swelling: Immediate symptoms following the trauma typically include pain and swelling at the site of the injury.
Tenderness: Palpable tenderness is often localized to the medial femoral epicondyle (the origin) or the distal attachment on the tibia.
Joint Laxity and "Giving Way": Because the MCL is a prime passive stabilizer against valgus forces, an injury leads to joint laxity. Patients may experience a sensation of the knee "giving way" due to this instability.
Loss of Motion: Patients often experience a loss of range of motion (ROM), specifically difficulty achieving full extension or flexion.
Neuromuscular and Functional Symptoms
Quadriceps Wasting and Weakness: A significant symptom following MCL injury—especially if the knee is immobilized—is quadriceps wasting, characterized by a decrease in the size and number of muscle fibers. This weakness often results in a knee extensor lag, where the patient is unable to fully extend the knee actively and walks with a flexed knee during the midstance phase of gait.
Loss of Proprioception: Damage to the ligament disrupts sensory feedback, leading to sensorimotor disorders and a decreased ability to sense joint position (proprioception).
Functional Limitations: Patients frequently have difficulty with basic activities of daily living, such as walking and climbing stairs, and are typically unable to perform more demanding athletic tasks like running, jumping, or pivoting.
Chronic Symptoms: In some cases, patients may experience persistent, refractory pain and activity limitations even after the initial healing period
Anatomy and Function of the MCL Ligament
The Medial Collateral Ligament (MCL) is the prime static stabilizer of the medial side of the knee. It belongs to a group of ligaments that act as passive stabilizers to guide and control knee motions while counteracting external forces.
Here's a breakdown of its anatomy and function:
Attachment Site: The MCL is approximately 8 cm to 10 cm long. It originates proximally on the medial femoral epicondyle and attaches distally to the tibia and the pes anserinus, roughly 5 cm to 7 cm distal to the joint line.
Structure: The ligament is divided into two distinct parts: the superficial MCL and the deep MCL. The deep layer is considered a thickening of the joint capsule and is further subdivided into meniscofemoral and meniscotibial components, both of which attach to the medial meniscus.
Functional Role in Stability: The primary role of the MCL is to stabilize the knee against valgus forces (stress pushing the knee inward). It works synergistically with other structures, including the posterior oblique ligament, the medial hamstring muscles, and the gastrocnemius muscle to maintain medial integrity.
Biomechanical Properties and Loading: The highest strains in the MCL occur when the knee is in full extension, at which point the forces are distributed evenly over the ligament. As the knee moves through various flexion angles, the forces are redistributed over different portions of the ligament.
Vascularization and Healing: Unlike the anterior cruciate ligament (ACL), the MCL is highly vascularized. This high blood supply provides the ligament with a good self-healing capacity, which often allows isolated ruptures to be treated non-operatively through functional rehabilitation.
Sensorimotor Role: Beyond its mechanical function, the MCL is vital for sensory feedback. It provides proprioceptive input that influences spinal motor reflex mechanisms, such as the H-reflex. A disruption of the MCL can lead to neuromuscular deficits, including altered muscle firing rates and quadriceps weakness, due to the loss of this feedback.
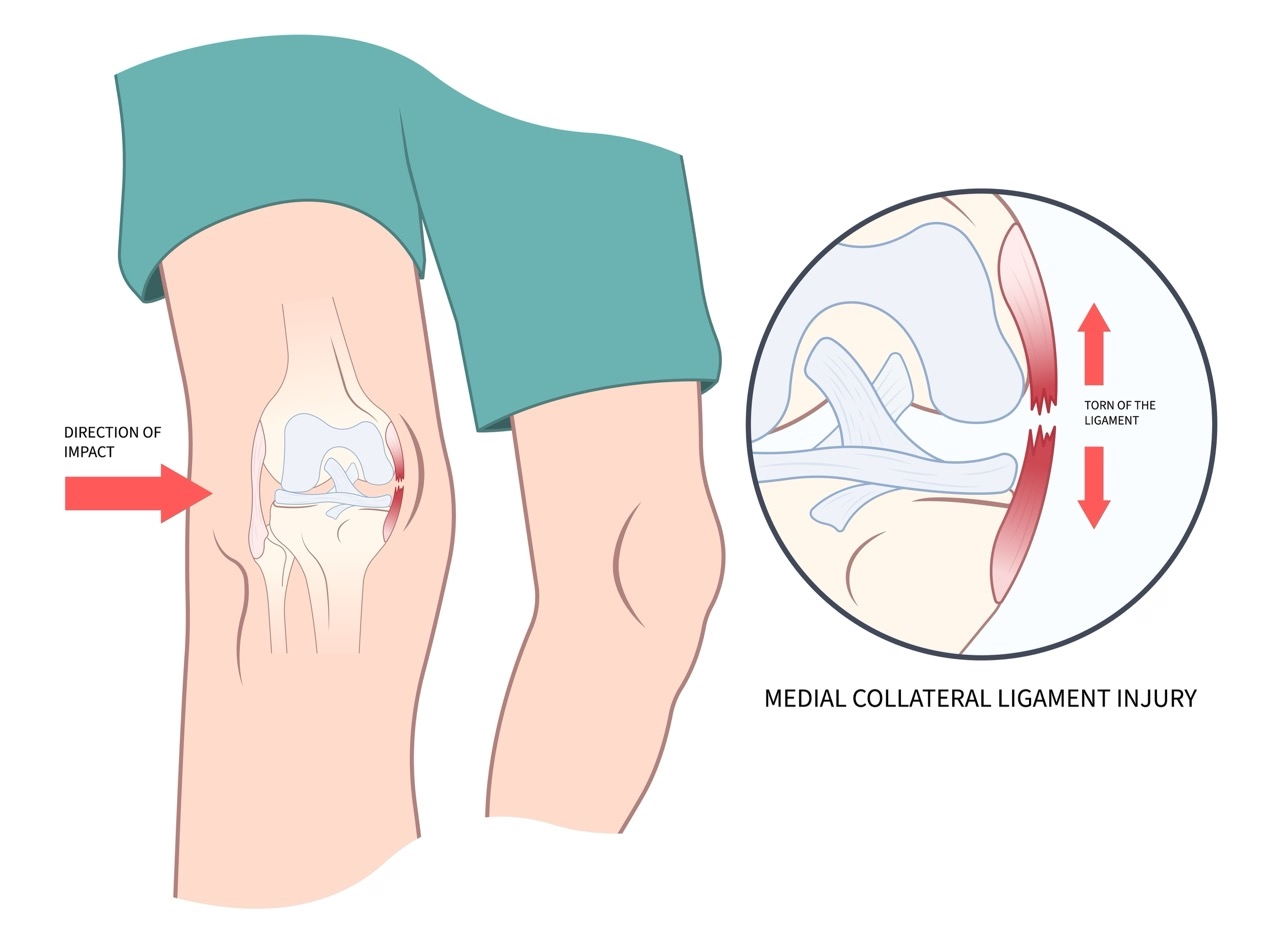
Injury Mechanism: The MCL is most susceptible to injury when the knee is subjected to valgus stress at approximately 20° of flexion, often combined with the external rotation of the tibia.
In summary, the MCL is a complex, multi-layered stabilizer essential for protecting the medial knee from valgus stress. Its unique anatomical attachments to the joint capsule and meniscus, combined with its high vascularity and role in neuromuscular signaling, make it a critical component for both mechanical joint stability and coordinated movement.
Causes and Risk Factors of MCL Sprains
The development of a Medial Collateral Ligament (MCL) sprain is primarily linked to acute traumatic events involving excessive force on the medial (inner) side of the knee. While it is not typically an overuse injury like tendinopathy, it is the most common ligamentous injury of the knee, particularly prevalent in high-impact sports.
Here are the key causes and risk factors for MCL sprains:
Traumatic Mechanisms of Injury:
Valgus Stress: The most frequent cause is a direct blow to the lateral aspect (outside) of the leg or knee, creating a valgus force that overstretches or tears the fibers on the medial side.
Non-Contact Landing: Landing from a jump in a way that sustains a severe valgus force at the knee can cause a sprain without direct impact.
Rotational Forces: Injuries frequently occur when the knee is at 20° of flexion subjected to valgus stress, often combined with simultaneous external rotation of the tibia.
High-Risk Sports: Athletes in sports involving pivoting, cutting, and contact—such as football (soccer) and American football—have a high prevalence. For example, an elite male football team can expect an average of two MCL injuries per season.
Anatomical and Biomechanical Factors:
Prime Static Stabilizer: The MCL is the prime static stabilizer against valgus forces; therefore, any force exceeding its tensile strength will lead to a Grade I, II, or III injury.
Anatomic Alignment: Individuals with pre-existing valgus alignment (knock-knees) in their normal stance may subject the MCL to higher baseline forces, potentially increasing susceptibility or complicating recovery.
Strain Distribution: The highest strains on the MCL occur at full extension, where forces are distributed evenly. As the knee flexes, forces are redistributed over different portions of the ligament, making it vulnerable at specific angles.
Neuromuscular Factors:
Loss of Proprioception: The MCL provides vital sensory feedback for knee stability. A previous injury or underlying deficit in proprioception can lead to sensorimotor disorders, making the knee less able to respond to destabilizing loads and increasing the risk of re-injury.
Altered Reflexes: Disruption of the MCL can alter the spinal motor reflex mechanisms (such as the H-reflex), which may lead to quadriceps weakness and further instability.
Associated Injuries (Combined Risk):
MCL injuries often occur in conjunction with other ligament tears. If a patient demonstrates medial instability in full extension, there is a high risk of concomitant ACL or PCL injury.
Combined ACL-MCL tears are common in specific activities, such as skiing, where the incidence ranges from 16% to 57%.
In summary, MCL sprains are typically the result of sudden valgus or rotational trauma. Risk is significantly elevated in contact sports, and individual factors such as limb alignment and neuromuscular control play a crucial role in both the susceptibility to injury and the success of subsequent rehabilitation.
Why Physiotherapy is Essential for MCL Sprain Recovery
Physiotherapy serves as the primary non-surgical treatment approach for the majority of isolated Medial Collateral Ligament (MCL) injuries. The overarching goal of physiotherapy is to restore joint stability, manage the ligament's inherent self-healing capacity, and reverse the neuromuscular deficits—such as quadriceps wasting and loss of proprioception—that follow the trauma, ultimately aiming for a safe return to sport or daily function.
Maximizing Healing through Early Functional Rehabilitation:
Unlike the anterior cruciate ligament (ACL), the MCL is highly vascularized, which provides it with an effective self-healing (cicatrization) process.
Physiotherapy facilitates this by balancing the need for protection with the necessity of motion. While a hinged brace may be used to protect against further valgus stress, prolonged immobilization is avoided because it causes deleterious effects, including quadriceps wasting, decreased bone mass, synovial adhesions, and joint stiffness.
For Grade I and II sprains, immediate weight-bearing and ambulation are encouraged as tolerated, as early mobilization is a feasible practice that may facilitate a quicker recovery and prevent arthrofibrosis.
Restoring Neuromuscular Control and Dynamic Stability:
The MCL is a vital prime static stabilizer that also provides critical sensory feedback for the knee. Disruption of the ligament leads to sensorimotor disorders and a significant loss of proprioception (the ability to sense joint position).
Physiotherapy employs a "clinical pathway" to restore dynamic stability. This involves neuromuscular training, such as balance activities, agility drills, and perturbation training (using roller boards or tilt boards), which provide the patient with experience dealing with destabilizing loads in a controlled environment.
These interventions teach the patient to recruit muscles—specifically the quadriceps, hamstrings, and gastrocnemius—with the proper force and timing to protect the knee subconsciously during functional activities.
Targeted Strengthening and Specialized Eccentric Loading:
To counteract quadriceps inhibition and weakness, physiotherapists implement a progression of open kinetic chain (OKC) and closed kinetic chain (CKC) exercises. CKC exercises, like squats and step-ups, are emphasized because they produce muscle recruitment patterns that simulate functional activities.
Recent evidence strongly supports the inclusion of early and progressive eccentric (lengthening) exercises. High-intensity eccentric rehabilitation has been shown to fully recover muscle relaxation properties and afferent responses without any apparent detriment to ligament healing or surrounding tissues.
Throughout the process, the progression of rehabilitation is individualized, depending on the injury grade (I, II, or III) and the patient’s specific functional limitations, such as knee extensor lag
Activity Modification and Protected Loading:
Physiotherapists guide patients through activity modification to control "adverse forces" on the knee, specifically protecting the healing ligament from valgus stress.
For Grade I and II injuries, immediate weight-bearing and ambulation are often encouraged as tolerated, which can facilitate a quicker recovery compared to prolonged immobilization.
For Grade III injuries, activity is more strictly modified, often involving restricted weight-bearing (e.g., toe-touch) for the first 3 to 4 weeks, depending on the patient's pain levels and clinical stability.
Bracing (typically a hinged long-leg brace) is used as an adjunct to activity modification to allow for early motion while preventing further valgus injury.
Addressing Altered Muscle Function and Inhibition:
Knee injuries frequently lead to quadriceps inhibition and wasting (a decrease in muscle fiber size), often resulting in a knee extensor lag. This causes the patient to walk with a flexed knee during gait.
Physiotherapy aims to restore motor control and strength through targeted exercises like quad sets and straight-leg raises.
Neuromuscular electrical stimulation (NMES) is utilized as a vital tool to augment quadriceps activation, retard muscle atrophy, and help the patient regain voluntary control of the muscle.
Improving Movement Patterns and Kinetic Chain Stability:
Comprehensive rehabilitation addresses muscles both proximal and distal to the knee. For example, hip extension and adduction exercises are used early on, while hip abduction is initially avoided to prevent unwanted valgus force on the healing MCL.
Physiotherapists focus on restoring proprioception and neuromuscular control so that patients learn to recruit muscles (quadriceps, hamstrings, and gastrocnemius) with the proper timing and sequence to prevent abnormal joint motion.
As the ligament heals, patients progress to agility drills (e.g., cutting, pivoting, and jumping) to improve reaction times and ensure the knee can safely handle the destabilizing loads encountered during sports.
Adjunct to Other Non-Surgical Treatments:
Progressive eccentric (lengthening) training is a cornerstone of modern MCL rehabilitation, as it has been shown to improve muscle afferent responses and fully recover muscle relaxation properties without harming the healing ligament.
For cases involving refractory pain or slow progress, adjunct medical interventions may be considered alongside ongoing physiotherapy. These include platelet-rich plasma (PRP) injections, corticosteroid injections for chronic symptoms, atelocollagen injections, or even hyperbaric oxygen therapy to accelerate recovery.
Prognosis: Recovery Timeline for Quadriceps Tendinopathy
Conservative Rehabilitation:
Isolated MCL injuries are primarily managed non-surgically due to the ligament's high vascularization and excellent self-healing (cicatrization) capacity. Historically, treatment focuses on functional rehabilitation rather than surgical repair, as recovery outcomes for isolated ruptures are similar between the two approaches.
Management typically involves early mobilization to avoid the deleterious effects of prolonged immobilization, such as quadriceps wasting and joint stiffness. For Grade I and II injuries, the protocol often includes immediate weight-bearing and ambulation as tolerated, along with strengthening exercises and bracing.
In the early stages of rehabilitation, non-operative treatment is highly successful, with reported success rates (excellent results in performance or clinical assessment) ranging from 70% to 98%.
Recovery Timeframes:
Grade I (Mild): Athletes typically experience a rapid return to activity, with an average of 10 days missed from training.
Grade II (Moderate): The average lay-off time for professional athletes is approximately 35 days (five weeks).
Grade III (Severe): Because these involve complete tears, recovery is more prolonged. Weight-bearing may be restricted for the first four weeks, and bracing is often required for six weeks.
◦ General Return to Sport (RTS): Across all non-operative cases, the RTS timeframe typically ranges from 3 to 12 weeks. Some studies specify a tighter window of 4 to 9 weeks depending on the bracing and rehabilitation protocol used.◦ Chronic or Refractory Cases: For patients with persistent pain after the initial healing period (e.g., symptoms lasting three months or more), adjunct treatments like platelet-rich plasma (PRP) injections or corticosteroids may be used to facilitate a return to sport
Persistent and Refractory Symptoms:
While most isolated MCL injuries heal well, some patients may experience persistent, refractory pain and activity limitations following the failure of initial non-surgical treatment.
If non-operative measures fail to provide relief, clinical outcomes can be addressed through surgical intervention or adjunct treatments such as platelet-rich plasma (PRP) injections, which have shown success in treating refractory pain specifically after low-grade injuries.
Long-Term Consequences:
One study evaluating conservatively treated MCL injuries over a 10-year period found that while overall results were good to excellent, Grade III injuries showed significantly inferior results in every clinical outcome assessment compared to Grade I and II injuries.
Chronic muscle impairments and sensorimotor deficits—such as altered reflex mechanisms and loss of proprioception—can persist for months or years after the initial injury, potentially leading to long-term functional instability if not addressed through a structured rehabilitation program.
Other long-term studies indicate that even a decade after injury, there may be no significant difference in clinical performance or valgus stability between those treated surgically versus non-surgically for certain isolated ruptures, though this is subject to the initial severity of the tear.
Factors Influencing Recovery (MCL)
Injury Grade and Severity:
The severity of the injury (Grade I, II, or III) is the primary determinant of the rehabilitation timeline and the necessary level of protection. Grade III injuries, involving a complete tear, typically require a significantly longer period of immobilization (up to 6 weeks) and a more cautious progression of weight-bearing compared to Grade I and II sprains.
Adherence to Standardized Rehabilitation:
Adherence to a structured, phase-based program that avoids overly aggressive early treatment is crucial to prevent the disruption of healing tissues.
Biomechanical Factors and Limb Alignment:
A patient's anatomic alignment—specifically a pre-existing valgus (knock-knee) bias—can significantly prolong recovery. In these cases, weight-bearing must be restricted (e.g., partial or toe-touch only) for the first few weeks to avoid placing adverse forces on the healing ligament.
Individual Healing Response and Injury Location:
The MCL’s high vascularity generally facilitates a strong self-healing capacity; however, the anatomic location of the tear influences the prognosis. Tearing at the femoral insertion typically heals well, whereas injuries on the tibial side or those involving a tibial avulsion (where the ligament folds into the joint) are often more problematic and may require surgical consideration.
Neuromuscular Compensation:
The success of recovery often depends on the patient's ability to develop compensatory muscle activity patterns—particularly in the quadriceps, hamstrings, and gastrocnemius—to maintain dynamic stability in the presence of ligamentous laxity.
Start Your Journey to
Better Health Today
Recover faster, move better, and feel stronger with expert physiotherapy. Our team is here to guide you every step of the way.
Injury Grading and Laxity: The first step involves classifying the severity of the injury (Grade I, II, or III) using a valgus stress test to measure medial joint space opening (ranging from 3–5 mm for Grade I to >10 mm for Grade III).
Anatomic Alignment: Assessing for valgus alignment (knock-knee stance) is critical; patients with this bias may require more restrictive weight-bearing (e.g., toe-touch only) during the first few weeks to avoid placing adverse stress on the healing ligament.
Gait and Extensor Lag: Analyzing gait mechanics is essential to identify a knee extensor lag, where quadriceps weakness or limited patellar glide causes the patient to walk with a flexed knee during the midstance phase.
Patellar Mobility: Evaluating the superior glide of the patella is necessary, as decreased mobility interferes with the quadriceps' ability to pull through the knee extensor mechanism
Strengthening Exercises
Early Quadriceps Activation: To counteract quadriceps wasting and inhibition, rehabilitation begins immediately with quad sets and straight-leg raises (SLR). High-intensity electrical stimulation is often used as a vital adjunct to regain muscle control and retard atrophy.
Eccentric Loading: Incorporating progressive, high-intensity eccentric (lengthening) exercises is a modern cornerstone for MCL recovery. These exercises have been shown to fully restore muscle relaxation properties and neuromuscular function without detrimental effects on ligament healing.
Kinetic Chain Integration (Hip/Glute Work): Exercises for the muscles proximal to the knee are initiated early to optimize movement patterns. While hip extension and adduction are encouraged, hip abduction with resistance must be avoided in the early phases to prevent creating a valgus force on the medial knee.
OKC and CKC Progression: Strengthening progresses from Open Kinetic Chain (OKC) exercises for isolated muscle strength to Closed Kinetic Chain (CKC) exercises (such as wall slides, mini-squats, and step-ups). CKC exercises are emphasized because they produce muscle recruitment patterns that simulate functional activities like jumping and running.
Neuromuscular and Proprioceptive Training: Once strength is established, the plan incorporates perturbation training (using roller boards or tilt boards) and agility drills (cutting, pivoting, and jumping) to teach the patient to recruit muscles with the proper timing and sequence to maintain joint stability
Manual Therapy
Patellar Mobilizations: Patients are encouraged to perform self-patellar mobilization exercises during the early phases of healing. This technique is essential for restoring superior glide of the patella, which is necessary for the normal functioning of the knee extensor mechanism. A decrease in patellar mobility can interfere with the quadriceps' ability to "pull through" the knee, leading to a knee extensor lag.
Soft Tissue Considerations: While the sources do not explicitly detail "deep tissue release," they emphasize that prolonged immobilization can lead to synovial adhesions, joint stiffness, and quadriceps wasting (a decrease in muscle fiber size). Consequently, early mobilization and patellar work are prioritized over traditional joint mobilizations of the tibiofemoral joint, which are rarely necessary for these injuries
Activity Modification
Controlling Adverse Forces: The central principle of activity modification for MCL sprains is the control of valgus stress (forces pushing the knee inward). During the initial phase of healing, it is critical to avoid any activity that overloads the fragile, vascularized granulation tissue forming at the injury site.
Substitution with Low-Impact Activities: To maintain cardiovascular and muscular endurance while protecting the healing ligament, high-impact activities (like running or jumping) are substituted with stationary cycling and swimming.
Cycling is considered an excellent exercise for developing endurance while minimizing stress on the tibiofemoral and patellofemoral joints.
Swimming is introduced once the patient can achieve full weight-bearing as a way to enhance muscular endurance without the risks associated with ground-impact forces.
Graduated Loading: Activities are modified based on the injury grade. For Grade I and II injuries, weight-bearing is typically allowed "as tolerated". However, for Grade III injuries or patients with a natural valgus (knock-knee) alignment, weight-bearing may be strictly restricted to "toe-touch" only for the first 3 to 6 weeks to allow the ligament to remodel without being stretched
Additional Considerations:
Graduated Loading and Weight-Bearing: All loading and weight-bearing exercises should follow a gradual and progressive sequence tailored to the injury grade. For Grade I and II injuries, immediate weight-bearing is often tolerated, while Grade III injuries may require restricted weight-bearing (e.g., toe-touch only) for the first 3 to 6 weeks to allow the fragile granulation tissue to mature. Progression should move from light resistance and high repetitions (to improve muscle endurance) to high-resistance, low-repetition exercises in the later stages of rehabilitation.
Pain and Progress Monitoring: Physiotherapists must take care to avoid overly aggressive treatment, which is clinically indicated by a prolonged increase in pain following a session or a regression in the patient's functional progress. Symptom resolution is also a key guide for clinical decision-making, such as determining when a patient can discontinue the use of a protective brace.
Control of Adverse (Valgus) Forces: A central tenet of MCL rehabilitation is the strict control of valgus forces (forces pushing the knee inward), especially during the early "fibroplasia" phase when healing tissue is vascularized and fragile. While early mobilization is encouraged to prevent stiffness, exercises that impart a valgus stress to the knee must be avoided.
Hip Muscle Integration and Precautions: To optimize the kinetic chain, hip extension and adduction exercises are initiated early in the program. However, hip abduction with resistance should be avoided in the early phases, as it can inadvertently create a valgus force on the medial side of the knee.
Neuromuscular Electrical Stimulation (NMES): In cases where significant quadriceps wasting or inhibition is present—often resulting in a knee extensor lag—the use of high-intensity electrical stimulation is a vital adjunct. NMES helps the patient regain voluntary motor control, retards muscle atrophy, and improves quadriceps strength more effectively than exercise alone in the early stages.
Early Eccentric Rehabilitation: Inclusion of progressive, high-intensity eccentric (lengthening) exercises is highly recommended. Research indicates these exercises are effective for restoring muscle strength and neuromuscular function without detrimental effects on the healing ligament or surrounding tissues.
Prevention Strategies for MCL Sprains
MCL sprains are typically acute traumatic events resulting from valgus stress or sudden rotational forces. Consequently, prevention strategies focus on enhancing the knee's dynamic stability and providing external protection during high-risk activities.
Neuromuscular and Agility Training:
The MCL provides critical sensory feedback for joint stability; therefore, training that enhances proprioception and neuromuscular control is a vital prevention tool.
Agility training (such as shuttle runs, cut-and-spin drills, and lateral sliding) can improve reaction times in the quadriceps, hamstrings, and gastrocnemius muscles, allowing them to better respond to potentially destabilizing loads.
Training on unstable surfaces (like roller boards or tilt boards) can help the body learn to automatically recruit muscles with the proper force and timing to prevent abnormal joint motion during athletic tasks.
Strengthen the Entire Kinetic Chain (Hip and Glutes):
To maintain knee stability, it is essential to address the entire kinetic chain, including muscles proximal and distal to the knee.
Strengthening the hip extensors and adductors—as well as the hamstrings and gastrocnemius, which act as synergists to the MCL—can improve the knee's ability to maintain dynamic stability under stress.
Developing these compensatory muscle activity patterns helps the leg manage forces that would otherwise overstretch the ligament.
Prophylactic Bracing in High-Risk Sports:
In high-impact contact sports like football, prophylactic bracing is a common strategy to prevent MCL injuries.
Studies have indicated that these braces can provide 20% to 30% greater resistance to a lateral blow, significantly reducing the risk of a valgus stress injury.
Custom-fit braces, in particular, have been found to provide the most protection when the knee is in full extension or mild flexion, the positions where the MCL is most vulnerable.
Avoid Overloading During Recovery:
For those with a history of injury, preventing recurrence requires avoiding "overly aggressive" return-to-play protocols.
Stresses should be gradually and progressively increased to allow the healing tissues to adapt to functional demands.
Monitoring for prolonged increases in pain or a regression in functional benchmarks is a critical clinical guide to ensuring the knee is not being subjected to "adverse forces" before it has regained sufficient strength.
FAQs
What is the difference between ACL, PCL, and MCL?
Below is a few points that explains the difference between the medial and lateral collateral ligament structures supporting the knee joint.
Comparison of MCL and LCL
The content below outlines the key differences between the Medial Collateral Ligament (MCL) and the Lateral Collateral Ligament (LCL) in terms of anatomy, function, healing capacity, and rehabilitation considerations.
Anatomical Location
MCL: Located on the medial (inner) side of the knee.
LCL: Located on the lateral (outer) side, forming part of the posterolateral corner.
Bony Attachments
MCL: Originates on the medial femoral epicondyle and attaches distally to the tibia and pes anserinus.
LCL: Originates on the femoral epicondyle and attaches distally to the fibular head.
Structure
MCL: Divided into superficial and deep layers; the deep layer attaches to the medial meniscus.
LCL: Often associated with the capsule, arcuate ligament, and popliteus tendon.
Primary Stability Role
MCL: Prime static stabilizer against valgus forces (forces pushing the knee inward).
LCL: Provides stability against varus forces (forces pushing the knee outward).
Injury Mechanism
MCL: Typically caused by a direct blow to the lateral side of the knee or a non-contact landing creating valgus stress.
LCL: Injuries result in increased posterolateral rotatory laxity and varus laxity.
Healing Capacity
MCL:Highly vascularized with excellent self-healing (cicatrization) capacity.
LCL: Sources focus on surgical repair or reconstruction (using allografts) for acute and chronic deficiencies.
Primary Treatment
MCL: Isolated injuries are primarily managed non-surgically through functional rehabilitation.
LCL: Acute injuries often require reattachment with suture anchors or primary repair.
Rehabilitation Precautions
MCL: Focuses on controlling valgus stress; hip abduction is initially avoided to protect the ligament.
LCL: Focuses on minimizing varus stress; hip abduction with resistance must be avoided.
Weight-Bearing Progression
MCL: Grade I and II allow immediate weight-bearing as tolerated.
LCL: Typically requires a partial weight-bearing gait for 4 to 6 weeks to minimize stress on the graft.
Is surgery usually required for an MCL injury, even if it is a complete tear?
No, most isolated MCL injuries—including complete Grade III tears—are managed non-surgically. This is primarily because the MCL is highly vascularized, which gives it an excellent self-healing (cicatrization) capacity. Studies have shown that recovery outcomes for isolated ruptures are often similar between surgical and non-surgical treatments, while non-surgical approaches avoid surgical complication risks.
However, surgery may be recommended in specific "problematic" cases, such as:
Tibial Avulsions: Where the ligament is pulled off the bone at its attachment to the tibia.
Stener Lesions: Where the torn MCL is folded into the medial joint or lies superficial to the pes anserine tendons.
Combined Injuries: When the MCL tear is associated with other ligament injuries, such as the ACL or PCL.
Persistent Instability: When a patient continues to experience symptoms or activity limitations after failing non-surgical rehabilitation
Detailed Biomechanical Assessment of Your Entire Lower Limb: We establish the exact severity of your injury (Grade I, II, or III) and assess for valgus alignment, which may require specialized weight-bearing restrictions. We also screen for concomitant injuries (such as ACL or PCL tears) and evaluate patellar mobility to prevent a knee extensor lag.
Customized Exercise Programs Based on Your Specific Grade of Injury: Whether you require immediate weight-bearing and ambulation for a Grade I/II sprain or a more protected, restricted weight-bearing phase for a Grade III tear, your program is tailored to your ligament's healing stage.
Advanced Manual Therapy Techniques for Pain Relief and Tissue Healing: We utilize targeted patellar mobilizations to restore superior glide, which is essential for proper quadriceps function.
Progressive Loading Protocols Tailored to Your Activity Goals: Our programs utilize a balance of Open Kinetic Chain (OKC) and Closed Kinetic Chain (CKC) exercises to safely increase tension on the remodeling ligament. We incorporate progressive, high-intensity eccentric (lengthening) training, which has been shown to fully recover muscle function and afferent responses without harming the healing tissue.
Regular Monitoring and Program Adjustment to Optimize Recovery: We track functional benchmarks—such as range of motion (ROM), quadriceps strength, and the elimination of valgus laxity—to determine when it is safe to progress or discontinue bracing.
Why Choose Our Clinic for MCL Treatment?
Evidence-Based Expertise
Treatment Protocols Based on the Latest Research: We integrate findings from the most recent systematic reviews (including 2024 BMJ research) to address the traditional "knowledge gap" in non-operative MCL management.
Specialized Training in Ligament Rehabilitation: Our approach is based on the scientific principles of ligament remodeling and the sequential phases of inflammation, proliferation, and fibroplasia.
Proven Track Record with Both Athletic and Non-Athletic Populations: We have experience managing everything from professional football injuries to everyday knee trauma.
Personalized Care
Individual Assessment of Your Ligament Condition: We provide custom bracing solutions, ranging from short-leg hinged braces for mild sprains to long-leg braces locked in extension for severe injuries, depending on your specific anatomical needs.
Custom Treatment Plans Based on Your Specific Needs: We account for your natural alignment and pre-injury activity levels to ensure your rehabilitation is relevant to your life.
Regular Progress Tracking and Program Modification: We use clinical pathways to identify and treat specific impairments like quadriceps wasting or loss of proprioception.
Comprehensive Recovery Support
Education About Managing Daily Activities: We provide guidance on controlling adverse valgus forces during your daily routine to ensure the optimum healing environment.
Guidance on Return to Sport/Exercise: Our protocols include advanced perturbation training (using roller boards and tilt boards) and agility drills to restore the dynamic stability needed for jumping, cutting, and pivoting.
Long-Term Prevention Strategies: We offer expertise in prophylactic bracing and neuromuscular training to reduce the risk of re-injury when you return to high-risk activities
Take the First Step Toward Recovery
Don't let an MCL sprain limit your activities or affect your daily life. Our experienced team is ready to help you build a strong foundation for lasting recovery.
Book Your Specialized Assessment Today:
Phone: 905-669-1221
Location: 398 Steeles Ave W #201, Thornhill, ON L4J 6X3


.webp)
.webp)
.webp)


.avif)




