Why Physiotherapy Is Critical for Patellar Bursitis Recovery
Physiotherapy is a cornerstone of the conservative management of patellar bursitis, playing a vital role in both symptom resolution and the prevention of recurrence. By integrating manual techniques, therapeutic modalities, and targeted exercise, it addresses the physiological and mechanical factors that drive bursal inflammation.
- Addressing Root Causes and Biomechanics
- Gait and Alignment Correction: For conditions like pes anserine bursitis, therapists focus on correcting valgus stress and internal rotation through neuromuscular retraining and gait analysis.
- Hip and Core Control: Strengthening the hip abductors, particularly the gluteus medius, is essential for managing iliotibial band (ITB) bursa inflammation by reducing dynamic valgus and femoral internal rotation.
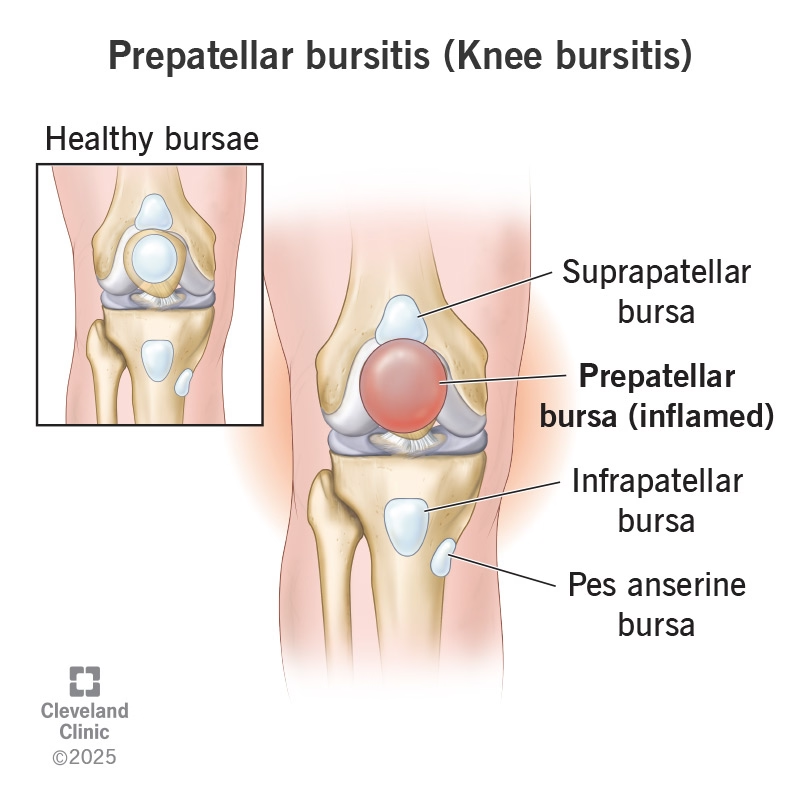
- Load Distribution: Addressing limb length discrepancies or poor foot mechanics helps redistribute pressure, preventing chronic compression of the prepatellar and infrapatellar sacs.
- Improving Tissue Mobility and Reducing Swelling
- Inflammation Control: Modalities such as ultrasound, cryotherapy (ice), thermotherapy, and iontophoresis are highly effective in reducing pain and synovial fluid overproduction.
- Preventing Adhesions: Unlike complete immobilization, which can lead to joint stiffness and the formation of adhesions around tendons, physiotherapy promotes controlled movement to maintain tissue health.
- Soft Tissue Release: Techniques like foam rolling or myofascial release help decrease tension on the patella, particularly for ITB-related issues.
- Restoring Strength and Functional Capacity
- Targeted Strengthening: Programs focus on the quadriceps, hamstrings, and hip abductors to ensure the knee joint is properly supported during high-impact activities like running or jumping.
- Flexibility: Stretching the hamstrings and quadriceps reduces the "pulley" tension on the patella, thereby decreasing the shear forces exerted on the deep and superficial infrapatellar bursae.
- Functional Stability: Therapy restores the stability required for essential daily tasks, such as climbing stairs or rising from a chair, which are often painful for bursitis patients.
- Activity Modification and Education
- Ergonomic Adjustments: Patients are educated on ergonomic work positions and the use of protective equipment, such as kneepads, to avoid direct pressure on the prepatellar bursa.
- Phased Return: For athletes, therapists guide the transition back to high-friction activities—such as downhill running or cycling—ensuring mechanics are optimized to prevent flare-ups.
What to Expect: Prognosis and Recovery Timeline
Recovery times vary significantly based on the type and severity of the inflammation:
- Acute Non-Septic Bursitis: In many cases, symptoms can subside completely within a few days to one week with proper treatment.
- Septic Bursitis: This requires more intensive medical management. Clinical studies show the time to achieve a sterile bursal aspirate typically takes 3 to 4 days, though full clinical recovery often takes longer.
- Chronic Bursitis: If inflammation persists, it can lead to fibrotic thickening, septations, or the deposition of calcium crystals, extending the recovery period to several weeks.
- Surgical Recovery: For patients requiring a bursectomy (open or endoscopic), the timeline for returning to work or normal activities is generally between 10 and 18 days
Factors Affecting Recovery
- Presence of Infection: Septic bursitis is a serious complication that may progress to cellulitis or abscesses if not treated with antibiotics.
- Systemic and Co-existing Conditions: Recovery may be slower in patients with diabetes, obesity, rheumatoid arthritis, or gout.
- Immunocompromised Status: These individuals are at a higher risk for septic bursitis and may require more aggressive treatment, such as intravenous antibiotics.
- Biomechanical Contributors: Unaddressed issues like valgus stress, limb length discrepancies, or tightness in the iliotibial band (ITB) increase the likelihood of recurrence
Management and Physiotherapy Strategies
- Conservative Foundation (PRICE): The standard approach includes Protection, Rest, Ice, Compression, and Elevation. Compressive dressings are typically applied for a minimum of three days.
- Avoiding Immobilization: It is critical to avoid complete immobilization, as this can lead to the formation of adhesions around tendons and joints, resulting in permanent stiffness.
- Physiotherapy Assessment: A thorough clinical exam includes palpation to locate the exact site of tenderness, testing active range of motion, and evaluating for biomechanical triggers like poor gait or malalignment.
- Therapeutic Modalities: Physical therapy often utilizes ultrasound, thermotherapy, cryotherapy, and iontophoresis to reduce pain and increase movement.
- Kinesiotherapy and Strengthening: Exercises focus on restoring muscle strength and range of motion, specifically targeting the quadriceps, hamstrings, and hip abductors to stabilize the knee.
- Biologic Options for Refractory Cases: For chronic cases that do not respond to standard care, the sources suggest that biologic therapies, such as Platelet-Rich Plasma (PRP) or PRP combined with hyaluronic acid, can provide anti-inflammatory and regenerative benefits to aid recovery
Exercise Prescription
- Early Stage: Protection and Activation
- Quadriceps Sets and Straight-Leg Raises: These exercises are fundamental for maintaining quadriceps tone when deep knee bending is painful.
- Glute Activation: Essential for controlling lower-limb alignment, particularly in cases where valgus stress contributes to bursitis, such as in pes anserine or ITB bursa inflammation.
- Avoiding Immobilization: The sources emphasize avoiding complete immobilization, which can lead to joint stiffness and the formation of adhesions around tendons.
- Middle Stage: Functional Loading
- Strengthening: Programs should target the hamstrings, quadriceps, and hip abductors to support the knee joint during load-bearing tasks.
- Controlled Squats and Step-ups: These help retrain the knee to handle compressive forces, though the sources suggest modifying squat depth if symptoms persist.
- Advanced Stage: Return to Sport and Impact
- Neuromuscular Control: Retraining gait and balance is critical for preventing the "shear forces" that irritate the bursae during dynamic activities.
- Sport-Specific Training: For athletes (e.g., volleyball players or runners), a phased return to jumping and running ensures the tissues have adapted to high-friction and high-impact stresses.
Therapeutic Modalities and Activity Modification
The use of modalities is supported as a "key role" in reducing pain and increasing joint ROM:
- Ice (Cryotherapy) and Ultrasound: These are primary tools for managing acute inflammation and synovial fluid overproduction.
- Shockwave Therapy (ESWT): While less common, the sources acknowledge its use in comparative studies for conditions like pes anserine bursitis.
- Activity Modification: This is the "silver bullet" of conservative care. Avoiding direct pressure—specifically repetitive kneeling—is mandatory to allow the synovial membrane to heal.
Preventing Recurrence: Long-Term Maintenance
Recurrence is common in patients who return to unmodified mechanical stressors. The sources suggest the following preventive pillars:
- Mechanical Correction: Addressing root causes like obesity, limb malalignment (genu valgum/varum), and poor gait mechanics reduces the "shear forces" between tendons and the bursae.
- Ergonomic Protection: For occupational kneeling (e.g., roofers, tile workers), the consistent use of kneepads and maintaining an ergonomic work position are essential for long-term prevention.
- Flexibility: Regular stretching of the hamstrings and quadriceps reduces tension on the patella and its associated bursae.
- Gradual Progression: Avoiding sudden increases in training volume or "overload" helps prevent the microtrauma that triggers chronic synovial hyperplasia
Our Specialized Approach to Rehabilitation
The rehabilitation of patellar bursitis requires a structured, multimodal strategy that balances the reduction of acute inflammation with the correction of long-term mechanical stressors. Based on the sources, a specialized approach to rehabilitation integrates the following evidence-based components:
Detailed Biomechanical Assessment
A thorough evaluation is critical because symptoms of bursitis often overlap with other conditions, such as patellar tendinopathy or meniscal tears.
- Mechanics and Alignment: Assessment includes identifying limb length discrepancies, foot pronation, and limb malalignment (such as genu valgum or varum), which increase pressure on specific bursae.
- Tracking and Provocation: Functional tests like the Noble and Ober tests are used to evaluate iliotibial band (ITB) tightness and compression.
- Imaging Integration: While diagnosis is primarily clinical, ultrasound is the preferred first-line tool to visualize synovial thickening or fluid accumulation, while MRI is reserved for evaluating deeper bursae or complex co-existing pathologies like osteoarthritis.
Customized Exercise Programs
The sources emphasize that exercises must be tailored to the specific anatomical site and the underlying driver of the inflammation:
- Prepatellar and Superficial Infrapatellar: Programs focus on avoiding direct pressure while restoring quadriceps and hamstring flexibility to reduce shear forces over the patella.
- Deep Infrapatellar: Because this bursa is influenced by tendon-bone mechanics, therapy targets quadriceps strengthening and activity modification to manage load during jumping and running.
- Pes Anserine and ITB: Focus is placed on hip abductor strengthening (specifically the gluteus medius) and gait retraining to correct dynamic valgus and femoral internal rotation.
Advanced Manual Therapy and Modalities
Physical medicine plays a "key role" in managing pain and promoting tissue health:
- Therapeutic Modalities: Evidence supports the use of ultrasound, cryotherapy (ice), thermotherapy, and iontophoresis to reduce synovial fluid overproduction and increase joint range of motion.
- Soft Tissue Techniques: Myofascial release and foam rolling are recommended, particularly for lateral knee pain associated with ITB friction.
- Swelling Management: The PRICE protocol (Protection, Rest, Ice, Compression, Elevation) is the gold standard for acute management, with compressive dressings often applied for at least three days.
Progressive Loading Protocols
Rehabilitation must find a "balance" between movement restriction and active recovery.
- Avoiding Immobilization: Complete rest is actively discouraged, as it can lead to joint stiffness and the formation of adhesions around tendons.
- Phased Recovery: Protocols involve a gradual transition from "relative rest" to sport- or job-specific tasks. For instance, occupational athletes (like roofers or carpet layers) are transitioned back to work with mandatory ergonomic protections, such as specialized kneepads.
Regular Monitoring and Advanced Interventions
- Frequent Re-assessment: Patients should be re-evaluated (typically every 48 hours in the acute phase) to monitor swelling, skin warmth, and the effectiveness of current therapies.
- Biologic Options for Resistant Cases: For chronic or refractory bursitis, a specialized approach may include biologic therapies like Platelet-Rich Plasma (PRP) or PRP combined with hyaluronic acid (PRP+HA). These offer anti-inflammatory and regenerative benefits that can improve pain and function more effectively than standard corticosteroid injections in resistant cases
FAQs
- Can patellar bursitis become chronic?
- Yes. Chronic bursitis can result from ongoing mechanical stress or inadequate treatment, leading to fibrotic thickening, septation, or pseudocapsule formation. Repetitive kneeling is a primary driver of this progression. Early intervention through physical medicine and kinesiotherapy is essential to restore range of motion and muscle strength, thereby reducing the risk of long-term irritation.
- Do I need imaging?
- Not usually. Diagnosis is primarily clinical, based on localized swelling and tenderness. However, ultrasound is the preferred first-line tool if confirmation is needed, as it allows for the visualization of fluid accumulation, synovial thickening, or signs of infection. MRI is reserved for complex, deep, or atypical presentations and is especially useful for differentiating bursitis from mimics like patellar tendinopathy or meniscal tears.
- Can I keep kneeling with patellar bursitis?
- Direct kneeling should be strictly avoided during the acute phase to reduce friction and allow the synovial membrane to heal. Once the inflammation subsides, occupational or athletic return requires the use of kneepads and ergonomic modifications to prevent the repetitive microtrauma that causes recurrence.
- Is surgery ever needed?
- Very rarely. Surgical treatment, such as a bursectomy (removal of the bursa), is restricted to severe, refractory, or chronic cases that have failed exhaustive conservative management. In the case of septic (infected) bursitis, a medical professional may need to perform surgical drainage if antibiotic therapy and repeated needle aspirations are insufficient.
- Can I still exercise?
- Yes, but modifications are mandatory. You should avoid complete immobilization, as it can lead to joint stiffness and the formation of adhesions. Instead, physical therapy focuses on a balance of movement restriction and active recovery. Initially, you must avoid high-impact loading (like jumping) and kneeling, but guided exercises like quadriceps sets and hip abductor strengthening help maintain stability without aggravating the bursa
Take the First Step Toward Recovery
Don't let patellar bursitis limit your activities or affect your daily life. Our experienced team is ready to help you build a strong foundation for lasting recovery.
Book Your Specialized Assessment Today:
Phone: 905-669-1221
Location: 398 Steeles Ave W #201, Thornhill, ON L4J 6X3
Online Booking: www.vaughanphysiotherapy.com
Serving communities across Thornhill, Langstaff, Newtonbrook, Willowdale, North York, Markham, Richmond Hill, Concord, and North Toronto.
Conveniently located in the heart of Thornhill, offering flexible scheduling to accommodate your recovery needs.
Created by Sara Lam
.avif)

.webp)
.webp)
.webp)


.avif)




