
Pelvic condition affecting pelvic floor strength, control, and function.
Pelvic floor dysfunction refers to a group of conditions in which the muscles of the pelvic floor do not function properly. These muscles support the bladder, bowel, and reproductive organs and help control urination, bowel movements, and sexual function. When the muscles become too weak, too tight, poorly coordinated, or injured, individuals may experience difficulties with bladder control, bowel movements, pelvic pain, or pressure in the pelvic region.
Pelvic floor dysfunction can affect people of all ages and genders, though it is more commonly reported in women due to factors such as pregnancy, childbirth, and hormonal changes.
Common Symptoms
Symptoms vary depending on whether the pelvic floor muscles are weak, tight, or poorly coordinated. Common symptoms include:
Symptoms can range from mild to severe and may worsen without appropriate treatment.
Prevalence
Pelvic floor dysfunction is a common condition. Studies estimate that up to one in three women will experience some form of pelvic floor disorder during their lifetime. It can also affect men, particularly after prostate surgery, chronic straining, or pelvic injury. Despite its prevalence, many individuals delay seeking treatment due to embarrassment or lack of awareness that effective treatments exist.
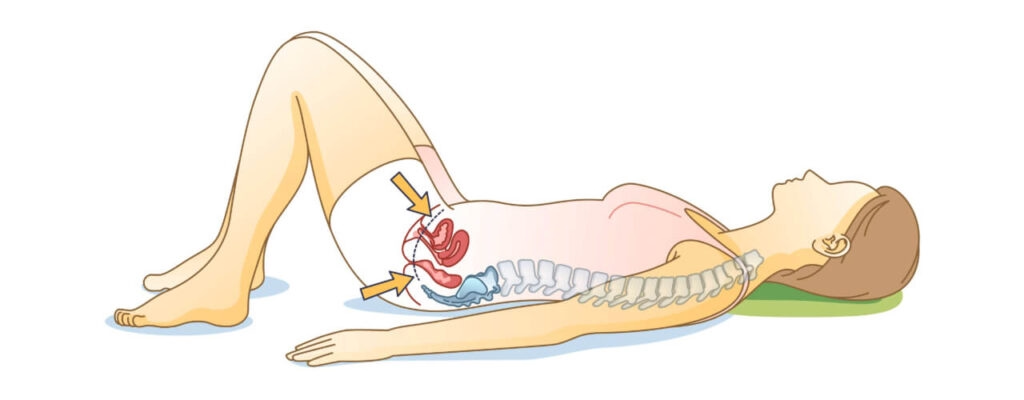
The pelvic floor consists of a group of muscles, ligaments, and connective tissues located at the base of the pelvis. These muscles form a supportive sling that stretches from the pubic bone at the front to the tailbone at the back.
Key functions of the pelvic floor muscles include:
When these muscles become weakened, tight, or uncoordinated, normal pelvic function can be disrupted.
The development of pelvic floor dysfunction (PFD) is a complex process often involving a combination of physical, biological, and behavioral stressors that disrupt the normal support system of the pelvic organs. When the pelvic floor muscles (PFMs) possess normal strength and tone, the pelvic organs are supported with minimal tension on the surrounding ligaments and fascia. However, when these structures are subjected to repeated stress, they can become stretched, weak, or hypertonic (excessively tight), eventually leading to clinical dysfunction.
The Mechanism of Gradual Development
Sources indicate that PFD often develops through a progression of stages rather than all at once:
Sources emphasize that because these conditions are often multifactorial, an effective recovery usually requires a multidisciplinary approach to address the various systems (muscular, fascial, and visceral) that have been impacted.
Recover faster, move better, and feel stronger with expert physiotherapy. Our team is here to guide you every step of the way.

Sources confirm that physiotherapy is the "cornerstone" of conservative management and a first-line, non-surgical treatment for pelvic floor dysfunction (PFD). Specialized pelvic health physical therapists utilize functional retraining to improve muscle strength, endurance, power, and relaxation, which is critical for reversing damage to muscles and connective tissues.
Specialized Assessment and Personalized Programs
A critical part of physiotherapy is a comprehensive assessment that evaluates the patient's ability to perform voluntary contractions and relaxations. This often involves the PERFECT scheme, a structured method to determine a personalized training effect based on:
Therapists also take a whole-body approach, assessing posture, gait, and the musculoskeletal, fascial, and visceral systems to identify all contributors to dysfunction.
Key Benefits of Physiotherapy
The Role of Early Intervention
Early intervention is particularly effective in the peripartum and postpartum periods. Performing antenatal pelvic floor exercises significantly reduces the risk of developing urinary incontinence both in late pregnancy and 3–6 months after birth. Furthermore, teaching patients "The Knack"—a well-timed voluntary contraction before a cough or sneeze—can provide immediate protection against leakage and prevent symptoms from worsening.
While it may take three to six months to fully train these muscles, research suggests that the benefits of physiotherapy are often maintained for years after treatment ends
The provided sources confirm that recovery from pelvic floor dysfunction (PFD) varies significantly based on individual factors, though they offer specific benchmarks for what patients can generally expect during their rehabilitation journey.
Prognosis and Recovery Timelines
Evidence suggests that muscle training and functional retraining are not immediate; it typically takes three to six months to fully train the pelvic floor muscles.
Factors Influencing Recovery
The success of the prognosis is heavily dependent on several variables:
Long-Term Outcomes
Most individuals experience significant symptom improvement that persists long after the active treatment phase.
Ultimately, the goal of management is to improve symptoms enough to maintain a normal lifestyle and restore confidence, allowing patients to return to social, employment, and leisure activities.
Sources strongly support the treatment approaches you listed, framing physiotherapy as a program of functional retraining designed to improve the strength, endurance, power, and relaxation of the pelvic floor muscles. These interventions are considered first-line, conservative treatments for a wide range of disorders, including incontinence, pelvic organ prolapse (POP), and chronic pelvic pain.
1. Pelvic Floor Muscle Training (PFMT)
PFMT is the "mainstay" of physiotherapy for pelvic dysfunction. It involves regular, maximum voluntary contractions and relaxations to "overload" the muscles, causing them to work harder or longer than normal to achieve a training effect.
2. Biofeedback Therapy
Biofeedback uses specialized equipment, such as vaginal or rectal pressure sensors, to provide audible or visual feedback on muscle activity. This is particularly critical for the one-third of women who are unable to correctly locate or contract their pelvic floor muscles on their own. It helps patients learn to either strengthen weak muscles or, in hypertonic cases, learn to fully relax them to reduce pain.
3. Manual Therapy
For patients with hypertonic (overly tight) pelvic floor disorders, hands-on manual therapy is pivotal. Techniques include:
4. Core and Postural Training
The pelvic floor muscles are integral to core stability at the base of the trunk. Research shows that a maximum pelvic floor contraction naturally triggers a co-contraction of the transversus abdominis (deep abdominal muscle), and training these together can produce a stronger effect. Therapists also address "pelvic pain posture"—such as excessive arching of the low back or rounded shoulders—which can chronically strain the pelvic floor.
5. Bladder and Bowel Retraining
Retraining strategies are used to restore a more normal voiding or defecation pattern.
6. Education and Lifestyle Modifications
Education is used to reduce anxiety and improve treatment adherence.
Additional Modalities
Sources also frequently highlight Electrical Stimulation—which uses a small current to help isolate and contract weak muscles—and Vaginal Weighted Cones, which patients hold in place during activity to promote reflex muscle activity.
Sources emphasize that preventing the recurrence of pelvic floor dysfunction (PFD) requires a combination of behavioral changes, lifestyle modifications, and long-term adherence to exercise regimens. Because PFD is often influenced by chronic environmental and physical stressors, ongoing management is necessary to protect the "trampoline effect" of the pelvic floor muscles and connective tissues.
Key Preventive Strategies
The Importance of Education and Awareness
Public and professional awareness is critical because many women incorrectly believe that pelvic floor symptoms are an inevitable part of aging or childbirth. Education empowers women to identify early "triggers" of dysfunction and seek intervention before symptoms become chronic. Furthermore, understanding that symptoms in one compartment (like the bladder) often affect another (like the bowel) allows for a more comprehensive approach to preventing a total relapse of pelvic health.
While significant improvement can be achieved within three to six months, maintaining these gains often requires a permanent lifestyle shift to avoid common pitfalls like boredom or forgetting to perform exercises, which are the primary reasons for low treatment adherence.
A comprehensive, patient-centered approach to pelvic floor rehabilitation is the "cornerstone" of conservative management, emphasizing that recovery depends on a systematic process of assessment, tailored intervention, and ongoing education.
1. Thorough Assessment
A thorough evaluation is critical because pelvic floor dysfunction (PFD) is often multifactorial, involving complex interactions between muscles, nerves, and connective tissues.
2. Individualized Treatment Plan
Effective rehabilitation is a program of functional retraining tailored to the objective findings of the initial exam.
3. Progress Monitoring
Regular follow-ups are essential to track improvements and address adherence, which is cited as a main influence on treatment success.
4. Education and Prevention Strategies
The goal of rehabilitation is to empower the patient with long-term habits that protect the pelvic floor.
This collaborative approach has been shown in controlled trials to significantly improve quality of life, restore social confidence, and often allow patients to avoid surgical intervention entirely.
Don't let pelvic floor dysfunction limit your activities or affect your daily life. Our experienced team is ready to help you build a strong foundation for lasting recovery.
Book Your Specialized Assessment Today:
Phone: 905-669-1221
Location: 398 Steeles Ave W #201, Thornhill, ON L4J 6X3
Online Booking: www.vaughanphysiotherapy.com
Serving communities across Thornhill, Langstaff, Newtonbrook, Willowdale, North York, Markham, Richmond Hill, Concord, and North Toronto.
Conveniently located in the heart of Thornhill, offering flexible scheduling to accommodate your recovery needs.
Created by Sara Lam
Explore the latest articles written by our clinicians
.webp)
.webp)
.webp)


.avif)




