
Pain in pelvic joints or surrounding muscles.
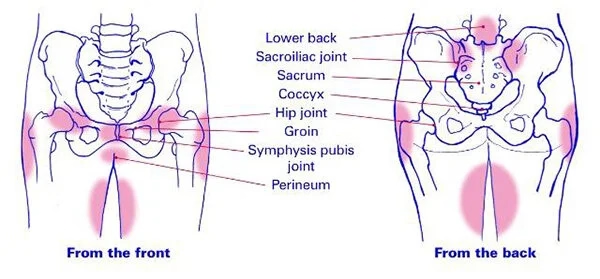
PGP is a musculoskeletal disorder primarily affecting the sacroiliac joints (SIJ), the pubic symphysis, and their supporting ligaments and muscles. It is specifically defined as pain between the posterior iliac crest and the gluteal fold, particularly near the SIJ, which may radiate to the posterior thigh and occur in conjunction with or separately from symphysis pain. PGP should be differentiated from general lumbar (low back) pain, which is typically concentrated higher up in the lumbar region.
Common Symptoms
Pain is often provoked by weight-bearing activities. Characteristic clinical signs include:
Prevalence
Sources indicate an incidence of roughly 20% during pregnancy. While most individuals recover after childbirth, sources provide a more nuanced long-term view:
The pelvic girdle is a ring-like structure composed of several bones and joints that provide stability and allow controlled movement.
Key anatomical structures include:
When these structures become irritated, unstable, or overloaded, pelvic girdle pain may develop.
The development of Pelvic Girdle Pain (PGP) is a complex process often involving a combination of physiological, biomechanical, and psychosocial factors.
Hormonal and Structural Changes
It is noted that PGP can debut as early as the 4th to 6th week of pregnancy, which is often before substantial biomechanical changes like weight gain or a shifted center of gravity occur. Furthermore, rather than general joint "looseness," it is specifically asymmetric mobility of the sacroiliac joints that is more strongly associated with the development of PGP.
Biomechanical Stress and Load Transfer
The pelvic girdle acts as a ring that must transfer loads from the spine to the lower limbs, a process requiring both form closure (stable joint surfaces) and force closure (compression from muscles and ligaments). Biomechanical dysfunction occurs when this load-transfer mechanism fails, often manifesting as:
Muscle Dysfunction and Motor Control
Altered motor control—the way the brain coordinates muscle activation—is a primary driver of PGP. This dysfunction typically falls into two categories:
History and Psychosocial Risk Factors
A history of previous lower back pain is a strong predictor for the development and persistence of PGP during and after pregnancy. Physical trauma, such as a significant fall on the buttocks, is also a known inciting event for non-pregnancy-related PGP. Additionally, sources highlight that psychosocial stress, including work-related stress and fear of movement, plays a significant role in how the condition develops and impacts a person's quality of life.
Aggravating Activities
Asymmetrical loading is a key provocateur. Symptoms are characteristically worsened by activities such as:
Physiotherapy is essential for managing Pelvic Girdle Pain (PGP) because it addresses the condition not just as a structural issue, but as a complex interplay of biomechanics, muscle activation, and patient beliefs. Research confirms that individually tailored physiotherapy focusing on body awareness and specific functional training provides a significant and lasting effect on pain, function, and quality of life.
Improving Pelvic Stability and Muscle Strength
Stability in the pelvis is achieved through "force closure," which is the compression generated by the coordinated activation of muscles, fascia, and ligaments. Physiotherapy targets these mechanisms in several ways:
Correcting Movement Patterns and Posture
PGP often leads to compensatory habits that further irritate pelvic structures. Physiotherapists use specific methods to restore normal function:
Reducing Pain and Inflammation
While exercise is critical, therapists also use manual techniques to provide symptomatic relief:
The Role of Education and Early Intervention
General Outlook and Postpartum Recovery
While PGP is often a self-limiting condition that improves after delivery, sources offer a detailed statistical breakdown of recovery:
Predictors of Persistent Symptoms
The recovery timeline is not the same for everyone; certain clinical indicators can predict whether PGP is likely to become chronic. According to sources, a poorer prognosis is associated with:
The Role of Targeted Physiotherapy in Recovery
Adherence to specific, tailored exercises is a major factor in the recovery timeline. Sources highlight that general exercise may not be sufficient for recovery, whereas specifically tailored programs show superior long-term results,,:
Recovery Timeline with Intervention
Sources suggest that while initial improvements can be seen relatively quickly, the full rehabilitative process often takes time:
Physiotherapy for Pelvic Girdle Pain (PGP) is characterized by an individualized, multimodal approach that addresses the specific biomechanical and functional needs of each patient. Because PGP can involve various underlying mechanisms—such as insufficient muscle activation or, conversely, excessive muscular "bracing"—treatment must be tailored to the specific subgroup the patient falls into.
Stabilization and Specific Exercise
While general exercise provides some relief, specifically tailored functional training has been shown to have a more significant and lasting effect on pain and quality of life.
Manual Therapy
Manual techniques are frequently used to address joint stiffness and soft tissue sensitivity.
Movement Retraining and Body Awareness
Restoring normal movement patterns is critical to preventing the "catching" sensation or the feeling that a leg might give way.
Education and Activity Modification
Education is often considered the most vital component of treatment to reduce fear and improve long-term outcomes.
Pelvic Support Belts
External supports like pelvic belts are often used to provide temporary compression and relief. However, their effectiveness varies:
Motor Control and Body Awareness
Preventing the recurrence of Pelvic Girdle Pain (PGP) relies heavily on maintaining specific motor control and body awareness rather than just general strength. While maintaining strong core and pelvic muscles is important, sources emphasize that specifically tailored functional training—which focuses on the coordinated activation of the transversus abdominis and pelvic floor muscles—has a more significant and lasting effect on preventing persistent pain compared to non-specific exercise.
Posture and Body Mechanics
Correcting an "increased sway" or lordotic posture can reduce the load on sensitive pelvic ligaments. This is often achieved through approaches like Mensendieck somatocognitive therapy, which trains patients in balanced posture and controlled movement patterns to avoid unnecessary muscular tension or "bracing".
Avoiding Prolonged Asymmetrical Loading
To prevent symptoms from returning, individuals should avoid prolonged asymmetrical loading, such as standing on one leg or twisting, as these movements are known to provoke pain in the sacroiliac joints and symphysis. Staying physically active with low-impact activities is beneficial, as studies have shown that aerobic exercises like fast-paced walking can significantly improve pain levels and psychological well-being.
Reassurance and Education
A gradual return to activity should be accompanied by reassurance and education, which help reduce the fear of movement and the mistaken belief that the pelvis is "unstable," both of which are factors in long-term recurrence.
Recover faster, move better, and feel stronger with expert physiotherapy. Our team is here to guide you every step of the way.

Physiotherapy for Pelvic Girdle Pain RecoveryPhase 1: Acute ManagementThe focus is on reducing pain and inflammation. Treatment may include rest, ice, compression, elevation (RICE), and modalities like TENS or ultrasound. Bracing or taping techniques may be used to offload painful structures and improve stability. Additional pain management strategies such as activity modification and analgesics can help control acute symptoms.Phase 2: Subacute RehabilitationGoals include restoring range of motion, gentle stretching, and initiating isometric strengthening exercises below the pain threshold. Manual therapy techniques such as joint mobilizations and soft tissue release may be incorporated to reduce pain, improve mobility, and address biomechanical restrictions. Dry needling may also be used to reduce muscle tension and modulate pain in the affected area. Both modalities are typically applied as adjuncts to exercise-based rehabilitation and are tailored to patient response.Phase 3: Strengthening and Functional RestorationIncorporates isotonic and eccentric exercises, balance training, and core strengthening to promote functional recovery.Phase 4: Return to FunctionSport- or work-specific reconditioning, with criteria-based progression for safe return to activities. Education on posture and ergonomic correction may also be provided.
Explore the latest articles written by our clinicians
.webp)
.webp)
.webp)


.avif)




