Post-Operative Meniscectomy Rehabilitation: A Physiotherapy Guide
What Is a Meniscectomy? Understanding the Procedure
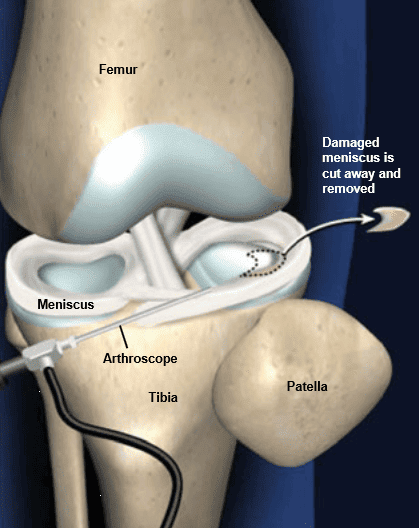
A meniscectomy—specifically a partial meniscectomy—is currently one of the most common orthopedic procedures performed when a meniscal tear is not suitable for repair.
What is the difference?
Partial Meniscectomy (Most Common)
Only the damaged or unstable portion of the meniscus is removed.
Goal: Preserve as much healthy tissue as possible to maintain long-term knee health.
Total Meniscectomy (Rare Now)
The entire meniscus is removed.
This is avoided when possible because it significantly increases the risk of:
Early osteoarthritis
Joint degeneration
Chronic pain
While the surgery addresses immediate symptoms like pain and locking, it fundamentally alters the knee's mechanics, meaning a structured recovery to prevent long-term degeneration
Common Post-Operative Symptoms
Pain is a primary symptom and typically manifests around the medial or lateral tibiofemoral joint line, especially during palpation or knee flexion activities.
In more extensive repairs or transplants, patients may also experience saphenous nerve irritation, characterized by burning sensations or hypersensitivity to light pressure and temperature changes along the medial thigh and knee.
Persistent joint effusion (swelling) is a common complication that must be monitored closely. Early control of this swelling is considered essential for effective pain management and the successful re-education of the quadriceps muscles. If left unmanaged, chronic effusion can lead to joint inflammation or even infection.
Stiffness is often most pronounced in knee flexion, and failure to meet specific ROM goals can lead to arthrofibrosis (the buildup of scar tissue).
Flexion: Patients may be at risk for flexion complications if 90° of motion is not easily achieved early on.
Extension: A loss of full extension (0°) is also a concern; therapists often use "overpressure" programs to prevent the knee from failing to reach a straightened position.
Patellar Mobility: Decreased movement of the kneecap (patella) is a significant contributor to overall joint stiffness.
The most significant muscular impact is quadriceps inhibition, often referred to as "quadriceps shutdown".
Strength Deficits: It is common to see quadriceps strength deficits of 20% to 40% as early as three weeks post-surgery.
Long-term Deficits: Without targeted strengthening, these extensors can remain significantly weaker than the uninjured limb for 12 weeks to even four years post-operatively.
Atrophy: This weakness is driven by rapid muscle atrophy resulting from the combination of pain, effusion, and the surgical procedure itself.
Early recovery is characterized by a necessary period of restricted weight-bearing to protect the healing tissue from high compressive and shear forces.
Gait Characteristics: Patients often display asymmetric gait patterns, such as limping or a "locked-knee" position during walking.
Prevalence
Arthroscopic meniscectomy is one of the most frequently performed orthopedic procedures worldwide. The annual incidence of meniscal injuries is estimated at 66 to 70 per 100,000 persons, reflecting its prevalence across both athletic and general populations.
Athletes: Traumatic lesions commonly affect athletes involved in high-impact activities. There is also a strong correlation between meniscal tears and other sports injuries; for example, 43% of patients with ACL injuries present with an associated meniscal tear.
Adults (30–60 years): In middle-aged men and women, the prevalence of meniscal injury ranges from 19% to 56%. These cases are often associated with degenerative changes and the early stages of osteoarthritis (OA).
Individuals with Mechanical Symptoms: Surgery is typically indicated when conservative management fails to resolve persistent mechanical symptoms like locking, catching, and "giving way" of the knee.
Anatomy of the Knee
Menisci and Articular Cartilage
The menisci are vital for shock absorption and stability. In addition to those primary functions, they are important for joint nutrition and proprioception as well.
Load Distribution: The menisci transmit 50% of joint compressive forces in full extension and up to 85% of the load in 90° of flexion
Position Sense: The meniscus provides a feedback mechanism for joint position sense (proprioception); its removal contributes to the "unsteady" feeling patients often report post-surgery
The health of articular cartilage is directly tied to the presence of the meniscus. Without the meniscus to distribute weight, the articular cartilage faces increased contact pressure, which is the primary driver of early joint degeneration and osteoarthritis. Clinical results for meniscal transplants are significantly better in patients with only mild cartilage damage compared to those with advanced deterioration.
Muscles Involved
The quadriceps and hamstrings do not just move the knee; they act as an active shock absorption system.
Following surgery, "quadriceps shutdown" occurs due to pain and swelling (effusion). This leads to rapid loss of muscle
Weakness in the quadriceps results in reduced shock absorption across the joint. When combined with the loss of the meniscus, this double-hit significantly accelerates the development of arthritis
Patellofemoral Joint
The patellofemoral joint (PFJ) is formed between two key structures:
Patella (kneecap)
A sesamoid bone embedded in the quadriceps tendon
Contains medial and lateral articular facets
Acts as a pulley to increase quadriceps efficiency
The trochlear groove of the distal femur
A V-shaped concave groove on the femur
Guides the patella (patellar tracking) during flexion and extension
Deeper grooves improve stability; shallow grooves increase risk of maltracking
Although the meniscus does not articulate directly with the patella, its role in tibiofemoral mechanics has a major influence on patellofemoral loading, tracking, and joint stress—especially post-meniscectomy.
Ligaments
Cruciate (cross-shaped) ligaments
Anterior cruciate ligament (ACL)
Attaches to the lateral the femoral condyle (side of the bottom of the hip bone) and the intercondyloid eminence of the tibia (top of the shin bone) Sits between the medial and lateral menisci.
The lateral meniscus has looser attachments, allowing more mobility—this is why ACL tears often come with lateral meniscus injuries.
The ACL helps control anterior tibial translation, which reduces shear forces on the menisci.
Posterior cruciate ligament (PCL)
Has close anatomical relationships with the medial meniscus.
Controls posterior tibial translation, reducing posterior shear and protecting the menisci from excessive compression.
Collateral ligaments
Medial collateral ligament (MCL)
Has a direct attachment to the medial meniscus (deep layer).
Because of this connection, valgus stress injuries that damage the MCL often injure the medial meniscus as well.
This attachment limits medial meniscus mobility, making it more prone to tears.
Lateral collateral ligament (LCL)
Does NOT attach to the lateral meniscus.
Instead, the lateral meniscus is separated from the LCL by the popliteus tendon.
The lack of direct attachment allows the lateral meniscus to be more mobile, decreasing its risk of injury compared with the medial side.
Causes and Risk Factors
Causes
A meniscectomy is typically required when a meniscus tear is considered non-salvageable or when conservative treatment has failed to resolve symptoms. While the current orthopedic consensus emphasizes preserving meniscal tissue whenever possible, the following specific conditions and clinical factors often result in the need for this procedure:
1. Nature and Location of the Tear
The primary factor in deciding on a meniscectomy over a repair is the blood supply and integrity of the tissue:
Avascular Zone Tears: The inner one-third of the meniscus lacks blood supply (the avascular zone), which prevents it from healing naturally. Tears in this region, particularly those with a rim width greater than 8 mm, are generally not suitable for repair and require removal.
Complex Fragmentation: If the meniscus has suffered major tissue fragmentation or degeneration, it cannot be structurally approximated or sutured back together.
Irreducible Tears: Tears with edges that cannot be properly reduced or aligned during surgery are candidates for removal.
2. Persistent Mechanical Symptoms
Surgery is often indicated when a tear causes significant dysfunction that interferes with daily life or sports. These symptoms include:
Joint "Locking" or Catching: Physical blockages caused by torn fragments moving within the joint.
"Giving Way": Instability of the knee during movement.
Chronic Pain and Effusion: Persistent swelling and pain on the joint line that does not respond to non-surgical interventions.
3. Failure of Conservative Management
A meniscectomy is frequently the "treatment of choice" when a period of conservative care (such as physiotherapy or activity modification) has failed to alleviate symptoms. Because the meniscus has low intrinsic regenerative potential, surgical removal may be the only way to provide rapid symptomatic relief and a fast return to work or sports.
4. Patient-Specific Contexts
Degenerative vs. Traumatic: In older populations (ages 30–60), tears are often degenerative and associated with early osteoarthritis. In these cases, if the damage is too extensive for repair, a partial meniscectomy is performed to smooth the joint surfaces.
Associated Injuries: Meniscal tears are highly prevalent in patients with other traumatic injuries; for instance, 43% of patients with ACL injuries have an associated meniscal tear that may require surgical attention
Risk Factors Leading to a Meniscectomy
1. Factors Increasing Injury Risk
Several demographic and activity-related factors increase the likelihood of sustaining the meniscal damage that precedes surgery:
Athletic and Physical Activity: Traumatic meniscal lesions are highly prevalent in athletes, particularly those in high-impact or pivoting sports. High incidence rates are also noted in specific active populations, such as military service members.
Age and Degeneration: In the general population, the prevalence of meniscal injury ranges from 19% to 56%, with middle-aged men and women being significantly affected. In these cases, tears are frequently associated with pre-existing osteoarthritis or general degenerative changes in the knee joint.
Concomitant Injuries: There is a strong correlation between meniscal tears and other knee traumas; for example, 43% of patients with ACL injuries also suffer an associated meniscal tear.
2. Factors Leading Specifically to Meniscectomy (vs. Repair)
Because modern surgical standards prioritize preserving meniscal tissue, a meniscectomy is typically chosen only when certain "risk factors" make a repair likely to fail:
Lack of Blood Supply (Vascularity): The most critical factor is the location of the tear. The inner one-third of the meniscus is avascular (lacking blood supply), giving it extremely low intrinsic regenerative potential. Tears in this "white-white" zone, or those with a rim width greater than 8 mm, are generally non-salvageable and require removal.
Nature of the Tissue Damage: Meniscectomy is often the only option for tears involving major tissue fragmentation, severe degeneration, or edges that cannot be surgically aligned (approximated).
Persistent Mechanical Symptoms: If conservative management (such as physiotherapy) fails to resolve symptoms like locking, catching, or "giving way" of the knee, surgical removal of the obstructive fragment is often indicated.
Start Your Journey to
Better Health Today
Recover faster, move better, and feel stronger with expert physiotherapy. Our team is here to guide you every step of the way.
Physiotherapy for Post-Operative Meniscectomy Rehabilitation RecoveryPhase 1: Acute ManagementThe focus is on reducing pain and inflammation. Treatment may include rest, ice, compression, elevation (RICE), and modalities like TENS or ultrasound. Bracing or taping techniques may be used to offload painful structures and improve stability. Additional pain management strategies such as activity modification and analgesics can help control acute symptoms.Phase 2: Subacute RehabilitationGoals include restoring range of motion, gentle stretching, and initiating isometric strengthening exercises below the pain threshold. Manual therapy techniques such as joint mobilizations and soft tissue release may be incorporated to reduce pain, improve mobility, and address biomechanical restrictions. Dry needling may also be used to reduce muscle tension and modulate pain in the affected area. Both modalities are typically applied as adjuncts to exercise-based rehabilitation and are tailored to patient response.Phase 3: Strengthening and Functional RestorationIncorporates isotonic and eccentric exercises, balance training, and core strengthening to promote functional recovery.Phase 4: Return to FunctionSport- or work-specific reconditioning, with criteria-based progression for safe return to activities. Education on posture and ergonomic correction may also be provided.
Team
Billy Tsakonas
Registered Physiotherapist MScPT · BSc. Kin Certified Vestibular Therapist

.avif)

.webp)
.webp)
.webp)


.avif)




