Why Physiotherapy Is Critical for Quadriceps Strain/Tear Recovery
Physiotherapy is critical for recovering from a quadriceps strain because the treatment and timeline vary significantly depending on the precise anatomical location and severity of the injury. A specialized approach ensures that high-risk "red flag" injuries are identified and that the muscle is properly remodeled to handle the explosive demands of sport.
Managing Pain and Swelling
The acute phase of physiotherapy (the first 24–72 hours) is focused on minimizing internal bleeding and edema through the RICE principle (rest, ice, compression, and elevation).
Restoring Safe and Full Muscle Length
Physiotherapy ensures muscle length is restored without risking a re-tear through "ballistic" or aggressive stretching.
- Graduated Stretching: Stretching is introduced in the active phase of management (3–5 days post-injury) and should only be performed to the point of discomfort, not pain.
- Passive ROM: A key criterion for beginning a running program is achieving full pain-free passive range of motion, typically tested in a prone position to compare against the uninjured leg.
- Active Warm-ups: Physiotherapists utilize active warm-ups to reduce muscle viscosity and activate neural pathways before rehabilitation exercises.
Rebuilding Strength through Controlled Progression
Strengthening exercises must progress sequentially to ensure the muscle can tolerate increasing loads.
- Exercise Hierarchy: Recovery moves from isometric contractions (no change in muscle length) to isotonic (shortening or lengthening against resistance), and finally to isokinetic and functional drills.
- Specific Milestones: For example, an athlete may be required to complete 3 sets of 10 single-leg hops pain-free before they are eligible to start a staged running program.
- Kicking Load: Because the rectus femoris is a "kicking muscle," rehab must include a graded reintroduction of kicking loads, starting with smaller, lighter balls before moving to full-intensity drills.
What to Expect: Prognosis and Recovery Timeline
The prognosis and recovery timeline for a quadriceps strain are heavily influenced by the precise anatomical location and the size of the injury, rather than just the clinical grade. While clinical grading provides a useful framework, research indicates that injuries involving the central tendon of the rectus femoris (the "red flag" diagnosis) require significantly longer rehabilitation intervals.
Recovery Timeline by Clinical Grade
Clinical grading, based on pain and loss of strength, helps guide early expectations:
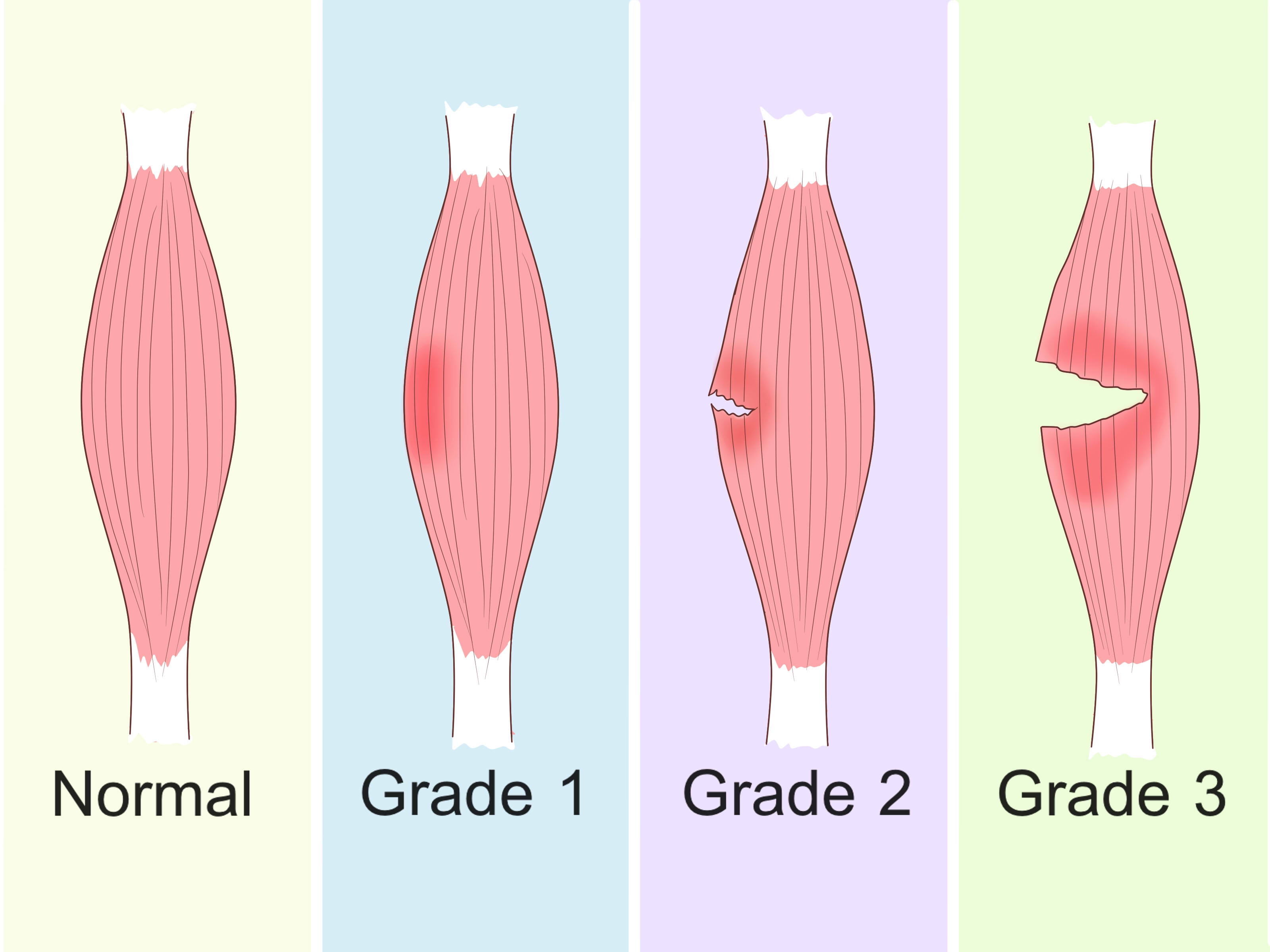
- Grade I (Mild): Involves minor tearing of muscle fibers with minimal to no strength loss. In professional athletes, peripheral or vastus muscle injuries—which often present as Grade I—typically resolve in 4.4 to 9.2 days.
- Grade II (Moderate): Characterized by more severe fiber disruption and noticeable weakness. Many significant rectus femoris injuries fall into this category, particularly those involving the central tendon, which average 26.9 days (approximately 4 weeks) of rehabilitation, with some cases extending to 43 days.
- Grade III (Severe): A complete rupture resulting in severe pain and a total loss of strength. While rare in professional settings, these injuries involve extensive rehabilitation and may require a surgical consultation if conservative management fails to improve function over several months.
Prognostic Factors: Why Location and Size Matter
Beyond the grade, the following factors are independent predictors of how long recovery will take:
- The "Bull's Eye" Lesion: Strains surrounding the central tendon of the rectus femoris are the most significant predictor of a protracted rehabilitation.
- Injury Length: Injuries 13 cm or longer average 20.6 days, compared to only 5.7 to 9.4 days for shorter lesions.
- Cross-Sectional Area (CSA%): Larger injuries (specifically those involving 15% or more of the muscle's cross-section) significantly increase the recovery time compared to minor strains.
- Site of Injury: Strains in the middle third of the muscle (averaging 16.2 days) typically take longer to heal than those in the proximal third (averaging 10.8 days).
General Recovery Expectations
- Acute Management (First 48–72 hours): Focus is strictly on the RICE principle (rest, ice, compression, elevation) to minimize internal bleeding and swelling.
- Walking and Mobility (1–2 weeks): Gait usually normalizes within the first two weeks as pain subsides. For contusions, recovery of a normal gait is a hallmark of "mild" severity.
- Running Progression (3–6+ weeks): An athlete is typically eligible to begin a staged running program once they achieve full pain-free passive range of motion and can complete 3 sets of 10 single-leg hops without pain.
- Return to Full Sport: Criteria for safe return include being entirely pain-free, having normal knee range of motion, and demonstrating near-normal strength compared to the uninjured side. In professional soccer, the average time loss for an index injury is between 18 and 21 days
Physiotherapy Treatment Approaches
Because the rectus femoris is a biarticular muscle with complex internal architecture, rehabilitation must be precisely phased to avoid shearing forces at the central tendon, which can significantly delay recovery.
1. Acute Phase (0–72 hours): Minimizing Damage
The primary goal is to minimize internal bleeding and edema to facilitate faster healing.
- RICE Protocol: Strict adherence to rest, ice, compression, and elevation is essential.
- Pain Management: Cryotherapy is effective for decreasing pain, while a short 3- to 7-day course of NSAIDs may be used. However, corticosteroids are discouraged as they can reduce the biomechanical strength of the healing muscle.
- Protection: For Grade 2 or 3 injuries, crutches may be necessary to facilitate initial immobilization and rest.
2. Subacute Phase: Restoration of Mobility
This "active phase" typically begins 3–5 days post-injury, depending on the severity.
- Restoring Length: Stretching must be graduated and pain-free; ballistic stretching is strictly discouraged to avoid re-tearing healing fibers.
- Activation: Soft tissue therapy and gentle isometric strengthening begin here to control pain and prevent atrophy.
- Prone Knee Flexion: A key milestone is achieving full, pain-free passive range of motion (ROM) in a prone position, which is used to compare the injured limb to the contralateral side.
3. Strengthening Phase: Building Resiliency
Exercises must progress sequentially to ensure the muscle-tendon unit can handle increasing tension.
- Sequential Loading: Progression moves from isometrics (contraction without length change) to isotonic (shortening/lengthening against resistance) and then isokinetic exercises.
- Milestones: Isotonic exercises (like leg presses or squats) are only initiated once isometric straight leg raises can be performed at multiple angles (0°, 20°, 40°) without pain.
- Muscle Hypertrophy: While early gains are neural, progressive loading over several weeks is required to address the decreased muscle volume and fascicle length common after injury.
4. Functional Phase: Sport-Specific Demands
In professional cohorts, a 4-stage running and kicking program is used to bridge the gap to full competition:
- Stage 1: 10 minutes of slow jogging.
- Stage 2: Striding at 40%–60% maximum with gentle stretching between sets.
- Stage 3: Sprinting at 90%–100% and the introduction of a staged kicking program, initially using a smaller, lighter ball for short distances.
- Stage 4: High-intensity sport-specific drills, including shuttle runs, figure-8 drills, and picking up/kicking the ball on the run.
5. Return-to-Sport (RTS) Criteria
The decision to return to sport is a collaborative one based on functional performance rather than time alone.
- Strength Symmetry: Athletes should demonstrate near-normal strength compared to the uninjured side; isokinetic testing is a valuable tool here.
- Functional Milestones: Before beginning the staged running program, the athlete must be able to complete 3 sets of 10 single-leg hops pain-free.
- Clinical Clearance: Full return is granted once the athlete can complete full team training both pain-free and with observed full function.
- Contusion Specifics: For contusion injuries, achieving 120° of knee flexion with the hip extended is a specific requirement for RTS
Preventing Quadriceps Strain/Tear Recurrence
Preventing the recurrence of quadriceps strains—which occur at rates of 15% to 19% in professional sports—is a critical component of long-term athletic health. Re-injuries are particularly problematic because they result in a significantly higher mean absence from training and competition than the initial injury.
1. Addressing the Strongest Risk Factors
The most effective prevention strategy begins with identifying those at highest risk. The there are three primary intrinsic risk factors:
- Prior History of Injury: A previous quadriceps strain is the strongest predictor of a future injury.
- Recent Hamstring Strain: Athletes who have sustained a hamstring injury within the previous 8 weeks are at a significantly higher risk for a subsequent quadriceps injury.
- Limb Dominance: In kicking sports, the dominant kicking leg is at a much higher risk due to the repetitive, high eccentric loads placed on the rectus femoris.
2. Managing Training Load and "Spikes"
External load variables are significant drivers of injury.
- Avoid Acute Spikes: Sudden increases in sprinting and kicking loads—common in the preseason following off-season deconditioning—greatly increase injury risk.
- Graded Reintroduction: Following an injury or a period of rest, therapists suggest a graded reintroduction of kicking, starting with lighter balls and shorter distances before progressing to full-velocity, sport-specific drills.
- Fixture Congestion: Monitoring fatigue during periods of "fixture congestion" (matches played within 5 days of each other) is vital, as increased muscle fatigue and decreased recovery time contribute to injury risk.
3. Optimizing Muscle Architecture and Strength
Rehabilitation must address the "maladaptive changes" that occur after a strain, such as decreased fascicle length, reduced muscle volume, and the development of scar tissue.
- Eccentric Loading: The rectus femoris is particularly susceptible to eccentric load. Chronic exposure to controlled eccentric loads that do not exceed the tissue's threshold may generate protective muscular adaptations.
- Strength Symmetry: Before returning to full activity, athletes should demonstrate near-normal strength compared to the uninjured side. Regular monitoring of strength throughout the season is recommended over a single baseline measure.
4. The Role of Flexibility and Warm-Up
- Flexibility Evidence: Interestingly, while often cited as a preventative measure, there is strong to moderate evidence that baseline flexibility has no significant association with future quadriceps injury risk. However, stretching remains a standard part of the "active phase" of rehab to restore functional length to the point of discomfort.
- Active Warm-Up: An active warm-up is critical before high-speed activity because it reduces muscle viscosity and activates essential neural pathways.
5. Specialized Care for "Red Flag" Injuries
Preventing recurrence is especially difficult if the initial injury involved the central tendon of the rectus femoris (the "acute bull's eye lesion").
- Protracted Rehab: These injuries require a significantly longer recovery period (averaging roughly 27 days) compared to peripheral strains (roughly 9 days).
- Optimal Remodeling: Professional athletes with intensive, supervised rehabilitation protocols for these injuries have shown zero recurrences, suggesting that "optimal remodeling" through graded exercise is the best defense against chronic pain and re-injury
Our Specialized Approach to Rehabilitation
1. Early But Safe Loading to Optimize Healing
There is a distinct two-phase approach to protect the initial healing of the muscle-tendon unit.
- The 48–72 Hour Window: Initial management focuses strictly on the RICE principle (rest, ice, compression, and elevation) to minimize internal bleeding and edema.
- Transition to Active Loading: A graded "remodeling phase" begins approximately 3 to 5 days post-injury.
- Threshold for Functional Work: Before transitioning to higher-impact loading (like the staged running program), patients must achieve full pain-free passive range of motion and be able to complete 3 sets of 10 single-leg hops without pain.
2. Evidence-Based Progression Tailored to Injury Grade
Rehabilitation timelines are not one-size-fits-all; they are dictated by the anatomical site and severity of the tear.
- The "Red Flag" Diagnosis: Injuries involving the central tendon (RF-CT), or "acute bull’s eye lesions," are critical to identify as they require a significantly longer recovery (averaging 26.9 days) compared to peripheral strains (averaging 9.2 days).
- Classification Systems: Progression is guided by established frameworks like the British Athletics Muscle Injury Classification (BAMIC), which categorizes injuries by site (myofascial, myotendinous, or intratendinous) and extent (Grades 1–4).
3. Manual Therapy and Neuromuscular Activation
Restoring the "kinetic chain" involves both mechanical and neurological interventions.
- Optimal Remodeling: Intensive physiotherapy, including soft tissue therapy, is used to ensure muscle-tendon junctions remodel optimally, which prevents the chronic pain and dysfunction often seen in less rigorous protocols.
- Activation Hierarchy: Strengthening moves sequentially from isometric (to restart neural firing without pain) to isotonic, isokinetic, and finally functional drills.
- Active Warm-Ups: These are prioritized to reduce muscle viscosity and activate vital neural pathways before high-intensity work.
4. Specialized Movement and Kicking Analysis
Because the rectus femoris is the primary "kicking muscle," your focus on movement mechanics is essential.
- Kicking Load Management: A staged kicking program that begins with smaller, lighter balls for short distances before progressing to full-velocity kicks with a normal-sized ball.
- Dynamic Functional Drills: Progressions include high-intensity drills such as shuttle runs, rapid change-of-direction (figure-8 drills), and picking up/kicking a ball on the run.
- Mechanics: Addressing altered running mechanics is vital, as injury can lead to maladaptive changes like decreased fascicle length and muscle volume that disrupt movement efficiency.
5. Return-to-Sport (RTS) Testing and Risk Mitigation
Clearing an athlete for sport is a multi-layered decision based on functional readiness rather than time.
- RTS Criteria: Athletes must be entirely pain-free, demonstrate near-normal strength compared to the uninjured side, and successfully complete full team training with observed full function.
- Targeting Risk Factors: To prevent the 15% to 19% recurrence rate, your approach addresses the primary risk factors: previous quadriceps injury, recent hamstring strain (within 8 weeks), and the unique demands placed on the dominant kicking leg
FAQs
- Should I stretch a quadriceps strain?
- Yes—but not during the first 24 to 72 hours. The initial acute phase requires strict adherence to the RICE principles (rest, ice, compression, and elevation) to minimize internal bleeding and swelling. You should keep the muscle relatively immobile during this window to allow for early healing.
- Once you reach the active phase (typically 3–5 days post-injury), you can introduce graduated stretching. It is critical that stretching is performed only to the point of discomfort, not pain, and ballistic (bouncing) stretching is strictly discouraged as it carries a high risk of re-tearing the healing muscle fibers. An active warm-up should always precede stretching to reduce muscle viscosity and activate neural pathways.
- When can I start running?
- The timeline depends heavily on the anatomical location and severity of the injury. While the average time-loss for an index quadriceps strain is 18 to 21 days, specific injuries vary significantly:
- Vastus muscle injuries: Average 4.4 days.
- Peripheral rectus femoris strains: Average 9.2 days.
- Central tendon ("Red Flag") injuries: Average 26.9 days (~4 weeks).
- You are generally eligible to begin a staged running program only when you meet two functional criteria: achieving full pain-free passive range of motion (compared to the uninjured side) and successfully completing 3 sets of 10 single-leg hops without pain.
- How do I know if I tore my quad instead of strained it?
- Clinically, a "strain" and a "tear" are part of the same grading spectrum. A Grade 3 injury (complete tear) is distinguished by:
- Severe pain and total loss of strength in knee extension and hip flexion.
- A palpable gap or defect in the muscle tissue, often detectable immediately after injury before swelling or a hematoma (fluid collection) obscures it.
- Significant swelling and eventual bruising, though ecchymosis (bruising) may not appear until 24 hours after the trauma.
- Is imaging necessary?
- While most injuries are diagnosed via clinical history and physical exam, MRI is considered the "gold standard" for characterizing injuries in professional athletes. It is particularly valuable for:
- Prognosis: Identifying the "acute bull’s eye lesion" (central tendon injury), which is a "red flag" diagnosis heralding a much longer recovery period.
- Clarification: Distinguishing between a strain and a contusion (direct blow), or identifying complications like myositis ossificans (bone formation within the muscle) in delayed recoveries.
- Refining Management: Measuring the cross-sectional area and length of the injury, both of which independently predict the length of the rehabilitation interval.
- Why do quad tears happen again so easily?
- Recurrence rates are high (15% to 19%) because an initial injury causes maladaptive changes in the muscle. These include:
- Structural Deficits: Decreased muscle volume, reduced fascicle length, and the development of scar tissue, which can interfere with the muscle's ability to tolerate loads.
- Persistent Weakness: Long-term deficits in muscle strength and neuromuscular inhibition often remain even after an athlete feels "functional".
- Inadequate Load Management: "Acute spikes" in loading—such as returning to full-velocity kicking or sprinting during the preseason or intense match play—can easily exceed the threshold of the remodeled tissue.
- Associated Injuries: A recent history of hamstring strain (within the previous 8 weeks) is a strong independent risk factor for sustaining a subsequent quadriceps injury
Take the First Step Toward Recovery
Don't let a quadriceps strain/tear limit your activities or affect your daily life. Our experienced team is ready to help you build a strong foundation for lasting recovery.
Book Your Specialized Assessment Today:
Phone: 905-669-1221
Location: 398 Steeles Ave W #201, Thornhill, ON L4J 6X3
Online Booking: www.vaughanphysiotherapy.com
Serving communities across Thornhill, Langstaff, Newtonbrook, Willowdale, North York, Markham, Richmond Hill, Concord, and North Toronto.
Conveniently located in the heart of Thornhill, offering flexible scheduling to accommodate your recovery needs.
Created by Sara Lam

.avif)

.webp)
.webp)
.webp)


.avif)




