MVA
Whiplash is the most common injury after a motor vehicle accident, and the assumption that it should clear up in a few weeks simply isn't borne out by the evidence. Across multiple studies, roughly 60% of people still experience persistent pain and disability six months after the original accident. Longer term, reviews have found that up to half of people continue to report symptoms a year out, and a meaningful subgroup carry severe, ongoing symptoms well beyond that.
So if you're still in pain at six months, you are squarely within the most common outcome, not an unusual one. When symptoms persist past this point, clinicians refer to it as chronic whiplash-associated disorder, or chronic WAD.
Statistic: About 60% of people still experience persistent pain and disability 6 months after a motor vehicle accident.
One of the most disheartening things patients hear is that because their X-ray or MRI looks clean, there's nothing physically wrong. But the research is clear that most people with whiplash show no visible structural damage on imaging, yet still develop real, lasting pain. In fact, one detailed study that put chronic whiplash patients through MRI with advanced spinal cord imaging found no structural lesions at the group level, even in those whose pain had become chronic. The absence of damage on a scan does not mean the absence of injury. It means the drivers of the pain are often things a standard scan isn't designed to show.
Researchers have identified several overlapping mechanisms.
Central sensitization. This is one of the best-supported explanations. After the injury, the nervous system can become hyperexcitable, amplifying pain signals so that even mild pressure or movement feels far more intense than it should. This heightened state can persist for months or even years past the acute phase. It shows up clinically as widespread tenderness, pain that spreads beyond the original injury site, and a lower threshold for pain when tested, all signs that the pain system itself has been turned up.
The stress connection is real and measurable. Recovery isn't purely mechanical. A large study following 740 whiplash patients over their first year found that those with high levels of post-traumatic stress symptoms early on were measurably more sensitized to pain at every single follow-up point, all the way out to twelve months. They also had more widespread pain, more headache and neck pain, and reduced neck mobility. The stress response and the pain system are biologically intertwined, which is a major reason an effective recovery plan treats the whole person rather than just the sore spot.
Soft tissue and muscle changes. Reduced neck movement, altered muscle control, and changes within the neck muscles themselves are commonly present early after whiplash and can persist over time in moderate to severe cases. These aren't signs of weakness or poor effort. They're part of how the body responds to the injury, and they're exactly the kind of thing targeted rehabilitation is designed to address.
.avif)
Certain factors make persistent pain more likely, and understanding them helps a practitioner build the right plan rather than place blame. Research has linked poorer recovery to higher pain intensity early on, high levels of distress or anxiety, a tendency toward pain catastrophizing (feeling overwhelmed or helpless about the pain), and having a pain condition before the accident. None of these are personal failings. They're simply useful signals.
Notably, the evidence does not support the common myth that people in compensation claims are somehow exaggerating. There is no clear evidence that being in a claim leads to worse outcomes.
Understanding that your pain has a real, identifiable basis is the first step toward addressing it. Conditions driven by sensitization, stress responses, and altered movement respond to active, structured rehabilitation: graded exercise, motor retraining for the neck and surrounding muscles, education about how pain works, and, where stress is a factor, approaches that address it alongside the physical recovery. Research on whiplash specifically has found that combining tailored exercise with stress-management strategies can reduce pain and disability more than exercise alone for those who need it. The aim is to gradually settle the overactive pain system and rebuild function, rather than chasing one symptom at a time.
.avif)
If your pain has continued for six months, there's a good chance your initial treatment was approved under the Minor Injury Guideline (MIG), the category Ontario's auto insurance system applies to sprains, strains, and whiplash. The MIG comes with a set limit on combined medical and rehabilitation benefits. For genuinely minor injuries that's often enough, but for the large share of people whose symptoms persist, that limit can be reached well before recovery is complete.
Here's what many people don't realize: injuries that turn out to be more than minor, including chronic pain conditions and certain psychological conditions that meet defined thresholds, may not belong in the MIG at all. Injuries that fall outside it can access substantially higher coverage. If your treatment has stalled because you've reached the limit of your current category, your classification is worth revisiting with a qualified practitioner.
A few other things worth knowing about how the system works:
Coverage after a motor vehicle accident comes through your own auto insurer under the Statutory Accident Benefits Schedule (SABS), and it's a no-fault system, meaning you're entitled to benefits regardless of who caused the crash. This coverage is separate from any extended health benefits you have through work, and you don't need a doctor's referral to begin treatment with a physiotherapist.
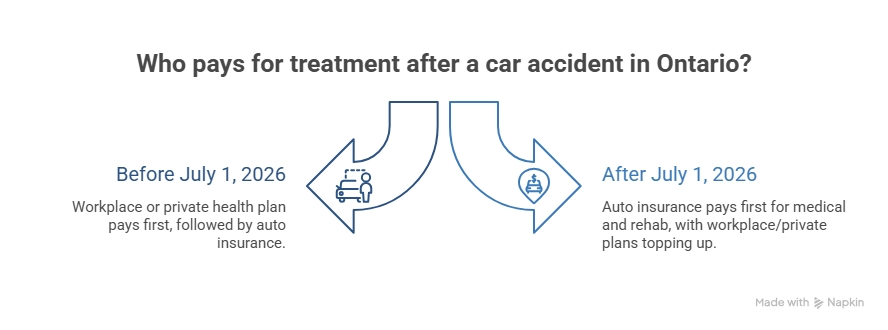
Ontario's accident benefits system is changing. For auto insurance policies issued or renewed on or after July 1, 2026, a new "first-payer" rule takes effect: your auto insurer must cover eligible medical and rehabilitation costs (other than medication) before your workplace or private health plan is tapped. Your extended health benefits can then top up anything auto insurance doesn't cover.
It's also worth knowing that for accidents that happened before July 1, 2026 with treatment continuing afterward, the existing rules continue to apply to that accident, so the system you started under generally stays with your claim. One thing that does not change: insurers still assess whether a proposed treatment plan is "reasonable and necessary," and a denied plan follows an established appeals process. A thorough, well-documented assessment from a qualified practitioner matters here.
Pain that lingers six months after an accident is real, it's common, and it has explanations rooted in how the body and nervous system respond to injury. A clean scan doesn't mean nothing is wrong, and persistent doesn't mean permanent. A proper reassessment of your injury, an active rehabilitation plan that accounts for the whole picture, and a clear understanding of what your coverage allows can together make a real difference in how you recover from here.
This article is for general information and isn't medical or legal advice. For guidance on your specific injury or insurance situation, speak with a qualified healthcare practitioner or your insurer.
Recover faster, move better, and feel stronger with expert physiotherapy. Our team is here to guide you every step of the way.

.webp)
.webp)
.webp)



